Abstract
Background
Total wrist replacement (TWR) as motion-preserving procedure continues to be critically discussed in the literature, although the complication rates have been significantly reduced with the current 3rd generation designs compared with older types. Possible reasons for this are often also a lack of knowledge about the currently available evidence, the complication management, and the lack of practical experience by the surgeons.
Methods
Based on an extended review of literature and own experience, the aim of this article is to give practicable insights for the clinician on: (1) biomechanical fundamentals, (2) differences in design, survivorship and functional outcome between the recent types, (3) possible pitfalls, and (4) failures and salvage options.
Results
The goal of TWR is that the overall wrist motion is maintained respectively improved despite it works with a locked midcarpal joint. Regarding survivorship and functional outcome the Maestro is (was) being superior over all other types that is (was) based on features in design. There is no scientific evidence as to why the Maestro was withdrawn from the marketplace by the company. For assessment of instability and/or impingement the use of dynamic radiographs is recommended. The problem of TWR is unchanged failure of the carpal components primarily based on mechanical dysbalance, and secondarily followed by metal and/or polyethylene wear, but surgical revision of asyptomatic periprosthetic osteolysis without safe radiagraphic signs of loosening is only required in not more than 20% of cases. For a failed TWR, revision TWR or conversion to total wrist arthrodesis are viable salvage options.
Conclusions
The knowledge about recent evidence and features in design of the available types, exact assessment of radiographic findings, presence of technical skills by the surgeons, and observance of the patient's expectations are the basic requirements for a successful TWR.
Keywords
Wrist, Osteoarthritis, Total wrist replacement, Survivorship, Functional outcome, Failure, Salvage options
Abbreviations
TWR: Total Wrist Replacement; TWA: Total Wrist Arthrodesis; PPOA: Painful Pancarpal Wrist Ostoeoarthritis; DRF: Distal Radius Fracture; DASH: Disability of Arm, Shoulder and Hand; PRWE: Patient-rated Wrist Evaluation; ADL: Activities of Daily Living; DRUJ: Distal Radioulnar Joint; CMCJ: Carpometacarpal Joint; UHR: Ulnar Head Replacement; USO: Ulnar Shortening Osteotomy; PE: Polyethylene; UTW: Universal Total Wrist; TCMJ: Thumb Carpometacarpal Joint; SLAC: Scapholunate Advanced Collapse; SNAC: Scapho-nonunion Advanced Collapse; PROMs: Patient-reported Outcome Measures; PPO: Periprosthetic Osteolysis; PEEK: Polyetheretherketone
Introduction
Total wrist replacement (TWR) is the motion preserving alternative to total wrist arthrodesis (TWA) for the first-line treatment of painful panacarpal wrist osteoarthritis (PPOA) for both rheumatic and non-rheumatic conditions (post-traumatic, primary PPOA, Kienböck’s disease, Gout), for the second-line treatment after a failed previously performed partial motion preserving procedure, for the first-line treatment of highly comminuted distal radius fractures (DRF) in single cases, and it can be useful as motion restoring procedure for patients who are unsatisfied after TWA and explicitly want wrist motion again (Figures 1-10) [1-14]. The goal of all modern 3rd generation TWR types (or 4th generation types if the Silicone implants are considered to be the 1st generation) compared to partial wrist fusion or proximal row carpectomy is the fact that wrist motion in summary is not impaired despite it works with a locked midcarpal joint [15].
Adams et al. [16] demonstrated impressively that in young healthy subjects limited wrist motion inevitably leads to statistically significant worsening of their ratings in Disability of Arm, Shoulder and Hand (DASH) and Patient-rated wrist evaluation (PRWE). In TWA patients, the lowest scores in activities of daily living (ADL) were found for perineal hygiene, using a screw driver, trouble using the hand in tight spaces such changing spark plugs on the family car, and followed by writing, drinking from a glass, turning a door knob, combing hair, and using a hammer (i.e. „dart-thrower‘s“ motion) [17]. Nearly all patients with TWA after a failed TWR reported in mid- to long-term outcomes, if given the chance, they would have a procedure again which is able to maintain wrist motion [18, 19]. A comparative study (TWR vs. TWA) at a mean-time follow-up of 68 months revealed that patients with TWR rated their self-reported outcomes significantly better than patients with TWA for both in DASH (29 vs. 38, p value 0.41) and PRWE (31 vs. 73, p value 0.01) [20]. Noted that not more than 60% of the maximum wrist capacity is needed to maintain functional wrist motion for ADL [21].
Limited or complete wrist or distal radioulnar joint (DRUJ) motion with or without pain is subsequently followed by impaired power and performance both in elbow and shoulder [16,22,23]. This pattern can be compensated by increased activities of trunk and shoulder muscles (upper trapezius and deltoideus) or using the other unaffected hand or both hands more often but over a not clearly known time [24-26]. The question is: are elderly patients with their age-related overall muscle degeneration able for this compensation mechanism, and if yes, how long, and what about the number of subsequently following functional disorders in elbow and shoulder in patients with longstanding impaired wrist motion?
The aim of this article content is to give practicable insights (tips and pitfalls) based on recent evidence and personal experience with the use of the ReMotion and Maestro implants over a period of 14 years.
Shortcomings and features in design
Historically, TWR utilizing older designs were associated with high complication rates especially due to mechanical failure of its carpal components, thus, it was mainly indicated for older patients with rheumatoid arthritis. With introducing of the recent 3rd generation TWR types Universal2 with it further development Freedom (Integra / Smith & Nephew, USA), ReMotion (stryker, USA) and both Maestro types with a higher modularity than the other implants (Zimmer Biomet, USA, withdrawn from the marketplace by the company in 2018) at the beginning of the 21st century the complication rates could be significantly decreased compared to the older types (0.1 - 2.9% vs. 0.2 – 8.1%), and there are no longer any significant differences compared to TWA (7% vs. 10%), but regardless of that TWA is performed nearly five times more frequently than TWR in USA [27-29]. Noted that Reigstad et al. [30] reported complication rates after first-line TWA with 60.5% at a long-term follow-up that is higher than previously assumed.
However, the main problem of the 3rd generation types is unchanged the long-term survivorship of its carpal component [6]. The simplification of the wrist by replicating contour and kinematics to a single radiocarpal articulation out of the physiological radio- and midcarpal joint leads to an unphysiological divergence between the center for extension-flexion and ulnar-radial deviation in the capitate that is followed by opposing rotational/translational contact pattern at the surface of both TWR components; and the circumduction ellipsis consisting of the coupled motion between the extension-flexion and ulnar-radial deviation arcs becomes smaller associated with the inability to obtain completely circumduction and the “dart thrower’s” motion as well as stress distribution like in a normal wrist [31-34].
The development of the semi-constrained resurfacing low-friction 3rd generation types (metal-on-polyethylene (PE) gliding), introduced by Menon in 1998 with the Universal total wrist (UTW) [35], with its anatomically shaped ellipsoidal articulations like a normal wrist and fixation of the carpal components with a central peg into the capitate (i.e. biaxial-anatomical) was the logical consequence in order to enhance stability compared to prior ball-and-socket types as well as to reduce the inacceptable high failure rate of the biaxial-physiological design (Biax). The Biax had an ellipsoidal articulation too but fixation of the carpal component with a peg into the 3rd metacarpal that often led to a breakthrough by the tip of the peg on the dorsal aspect [36, 37]. The rationale behind this specific complication is the anatomically predetermined longitudinal/transversal concavity of the metacarpus/carpus to volar that makes the dorsal cortices significantly less resistant to long-lasting load peaks („Wolff’s law“ 1892: bone trabeculae were arranged in response to the stress lines resulting in bone reinforcement at the pressure side and bone resorption at the tension side) [38]).
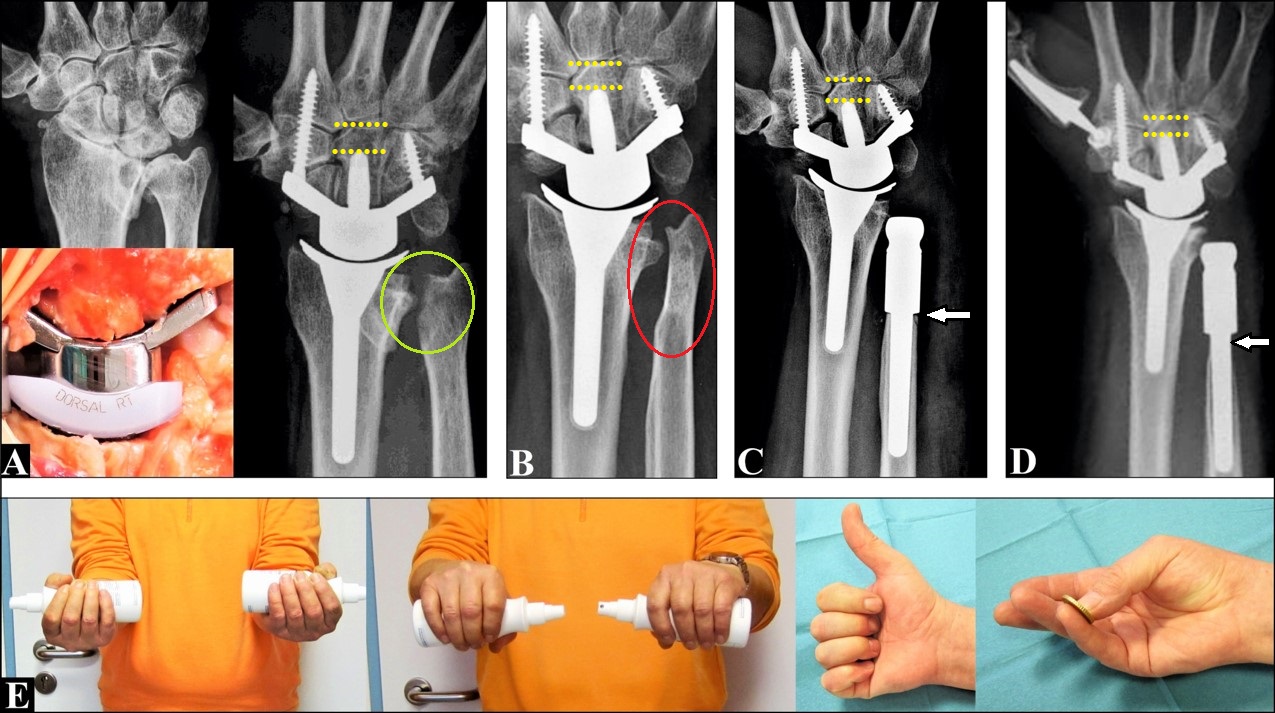
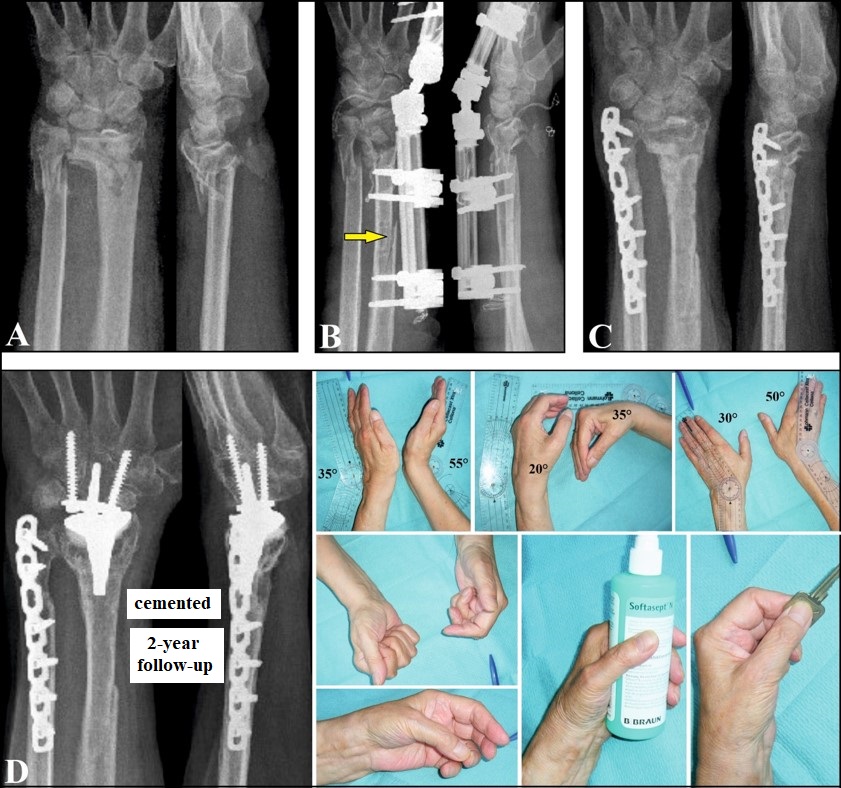
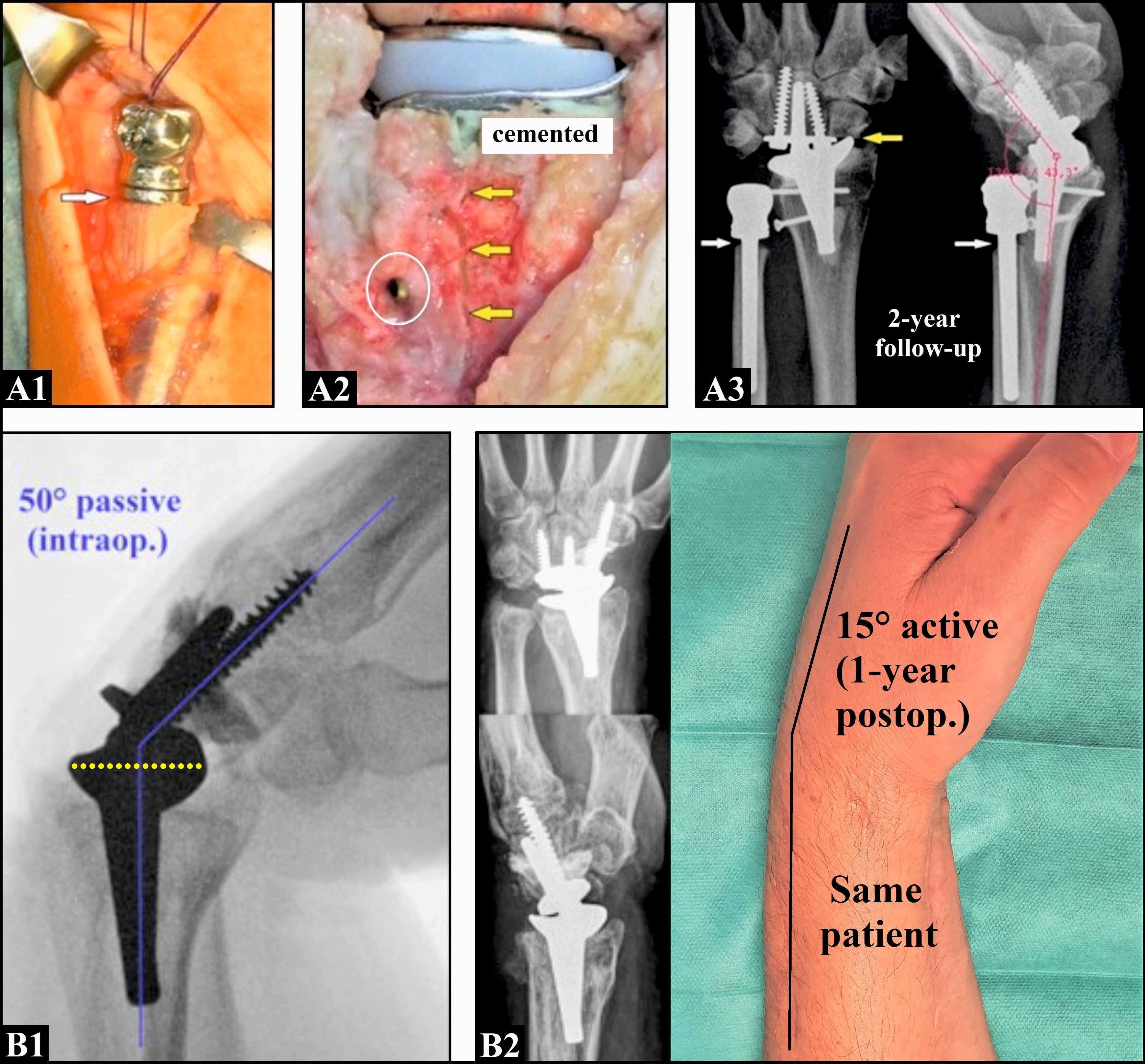
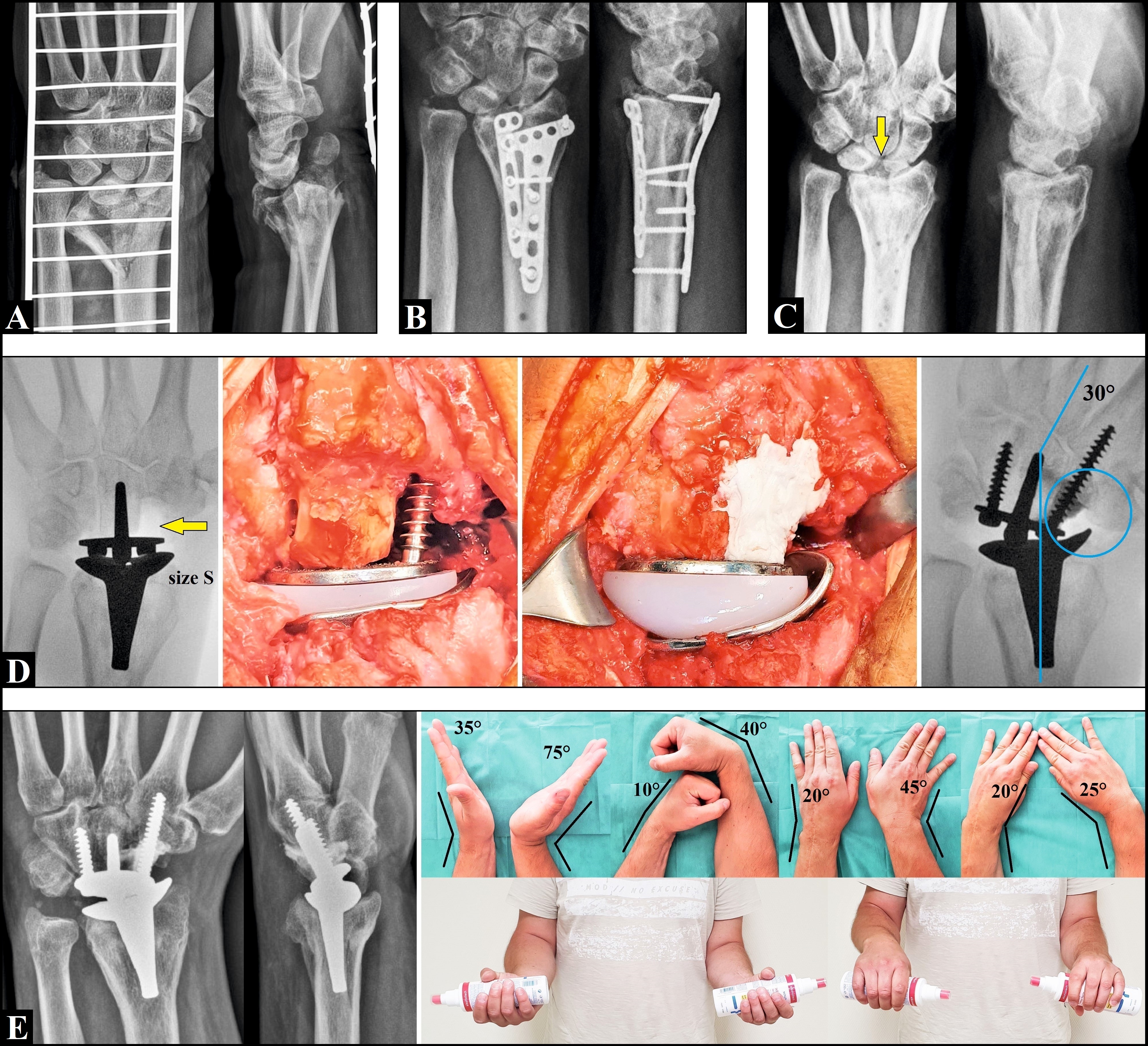
(All three patients received the 2nd Maestro type (locking screws for fixation the carpal components with scaphoid augments after removal of the entire scaphoid (white arrows) [14]): (A) This 79-year-old female sustained a left highly comminuted DRF with pronounced impaction of the distal radius metaphysis associated with poor osteoporotic bone stock. The primary cemented TWR combined with ulnar shortening and a cementless UHR utilizing the uHead prosthesis was performed. The course was complicated by development of distal radioulnar synostosis (two yellow arrows) that led to restriction of the supination-pronation motion arc, the forearm was completely fixed in 90° neutral position. (B) This 84-year-old female sustained a right highly comminuted DRF with impaction of the distal radius associated with poor osteoporotic bone stock as well. The primary cemented TWR combined with the Darrach procedure was performed. (C) This 56-year-old male sustained a left highly comminuted DRF with impaction of the distal radius metaphysis associated with good bone stock. The primary cementless TWR combined with an ulnar shortening osteotomy (USO) utilizing a 2,5 mm locking titanium plate was performed. Note the locking green colored polyaxial and blue colored monaxial fixation screws for the carpal plate.
{kind=link}
(55-year old male, right advanced stage of primary (or rheumatoid?) wrist and DRUJ arthritis [14], the further course is demonstrated in Figures 9A-E).: (A) The primary cementless TWR utilizing the 1st Maestro type (non-locking screws for fixation the carpal component, a resection at the proximal pole of scaphoid was done and therefore, the carpal component has no scaphoid augment) combined with the ulnar head hemiresection (Bowers procedure, green circle) was performed. The two yellow pointed lines mark the distance between the tip of the capitate peg and the CMCJ III. (B/C) Three years after surgery, a painful convergence instability occured (red oval circle) that required a conversion to an UHR. The uHead prosthesis with a long revision stem was pressfit inserted on the top of the distal ulnar stump (white arrow). The carpal component of the Maestro implant was not subsided (two yellow pointed lines). (D) Five years after surgery, both implants were not loosened. Typically, asymptomatic PPO around the collar of the UHR was observed (steady state, white arrow), the carpal plate of the Maestro implant was unchanged not subsided (two yellow pointed lines), and an additional total TCMJ replacement with the Arpe prosthesis was performed six months after UHR. (E) At the 5-year follow-up, the patient was unchanged pain free and very satisfied with his functional outcome.
{kind=link}
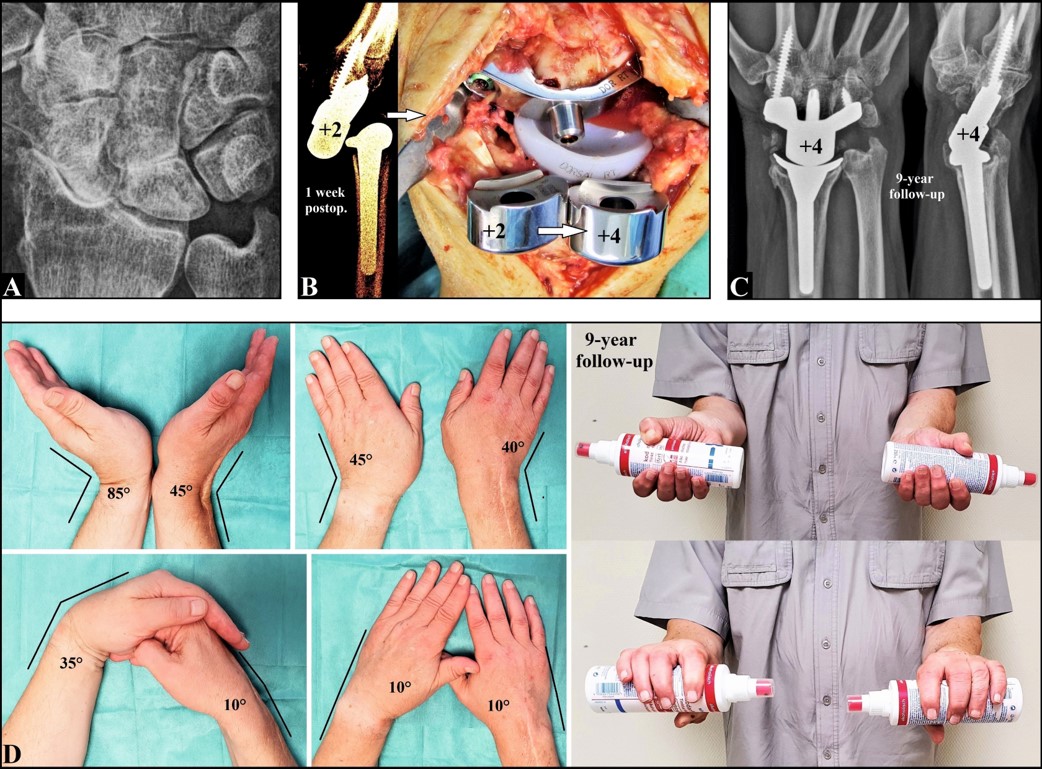
[14]: (A) A 55-year old male presented with right advanced stage SLAC primarily treated by a cementless TWR utilizing the 2nd Maestro type. (B) One week after TWR, an atraumatic dislocation of the Maestro implant in volar direction occured despite immobilization of the forearm with a plaster splint. For improvement the resection-related loss of carpal height (longitudinal alignment), a revision with exchange of the primarily inserted carpal head size 2 to size 4 without the necessity of an exchange procedure of the entire carpal component was performed (white arrow, note that with the use of the 1st Maestro type the entire carpal component had to be replaced). (C) At the 9-year follow-up, the implant was unchanged stable and not loosened. (D) The patient is unchanged pain free and very satisfied with his functional outcome, but note the marked decreased flexion compared to his left unaffected wrist
{kind=link}
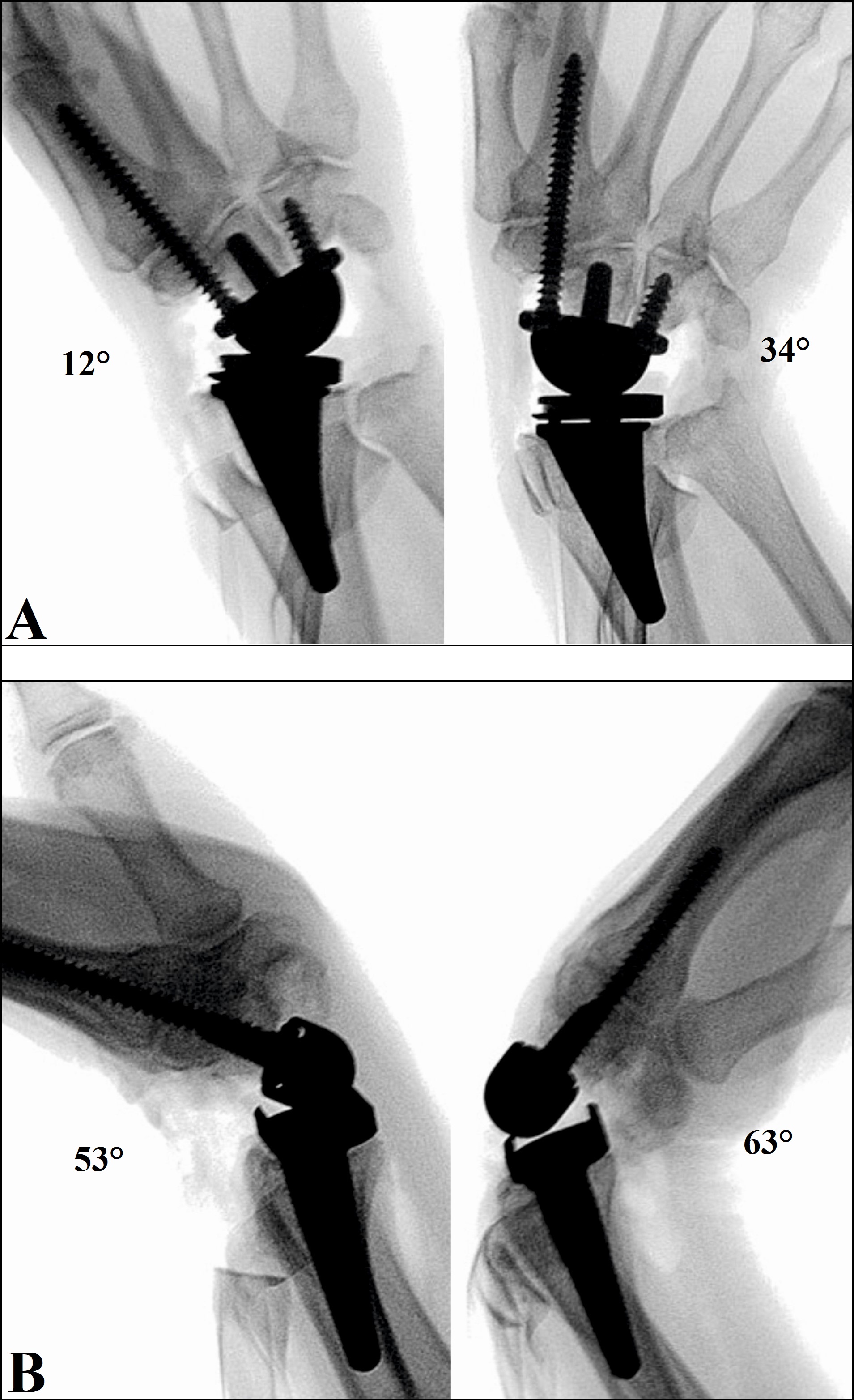
If a TWR is being considered, pre-operative evaluation of concomitant injuries or disorders at the DRUJ and/or thumb carpometacarpal joint (TCMJ) should be done (Figures 1,2,6,8,9). It is recommended to preserve the ulnar head because it serves as a cantilever for the entire wrist [7,8,12,39]. If the ulnar head is removed, as commonly done for rheumatic patients, there is potential risk for instability of the entire wrist or a TWR [40-42]. Dislocation of a TWR was mainly a concern with the older types observed in up to 9% of cases, but it may also occur with the recent 3rd generation types by iatrogenic injury of the volar extrinsic stabilizers of the wrist (radioscaphocapitate and long radiolunate ligaments) or insufficient restoration of resection-related loss of carpal height potentially leading to ligamentous instability of the entire wrist (Figure 3), and a suggested instability can often only be verified under dynamic test conditions [1,43]. One disadvantage of the UTW and Universal2 was/is that the DRUJ can be mechanically compromised by the radial component, caused by the required oblique resection in ulnar direction at the joint surface for placement of it (in contrast to the ReMotion and Maestro), that often required an ulnar head resection. Noted as well that pre-existing pronounced ligamentous instability presented as volar dislocation of the wrist in rheumatic patients is to be considered as contraindication for TWR [44].
[14]: (A) A 71-year-old female presented with a highy comminuted left distal forearm fracture associated with poor osteoporotic bone stock. (B) Primary external fixation was done. During the first attempt of external fixation an additional iatrogenic fracture at the radius shaft occured (yellow arrow) that required revision with re-placement of external fixation. (C) Six weeks thereafter, timely fracture healing was observed that makes the cemented TWR utilizing the ReMotion implant possible. (D) At the 2-year follow-up there was unchanged a correct positioning of the ReMotion implant without any signs of loosening, and the patient is unchanged pain free and very satisfied with her functional outcome.
{kind=link}
Regarding the placement of the two fixation screws for the carpal components there is a consensus in the literature that, in order to avoid micromotions at the screw-bone-interface as potential risk factor for loosening, the ulnar-sided screw should be placed only into the hamate whereas the radial-sided screw can be placed into the 2nd metacarpal with crossing the carpometacarpal joint (CMCJ) II [1]. This consensus is based on the predetermined joint anatomy which reveals a higher stability in the CMCJs II/III (i.e. stable amphiarthroses) compared to the CMCJs IV/V [45,46]. If a placement of the ulnar-sided screw into the 4th metacarpal would become necessary then the CMCJ IV arthrodesis should be considered with the use of bone graft. A potential advantage of the Maestro is (was) the possibility for use of a carpal plate involving a scaphoid augment associated with complete removal of the entire scaphoid that provides a stable support onto the bases of the trapez/trapezoid and may avoid the fusion of the surrounding carpal bones (Figures 1,3,6B1/2,10) [47].
(A1-3) A 62-year-old male presented with advanced stage of left SLAC and concomitant DRUJ arthritis, primarily treated by an UHR. The uHead prosthesis was pressfit inserted on the top of the distal ulnar stump (white arrow, A1). The UHR was followed by TWR six months later. During primarily cementless placement of the ReMotion implant with standard horizontal resection at the scaphoid, a large longitudinal periprosthetic fracture at the dorsal aspect of the distal radius metaphysis occured (yellow arrows) that required revision with a cemented re-placement combined with a osteosynthesis using two 3.5 mm titanium compression screws (white arrow, A2). At the 1-year follow-up, an uneventful course was observed, but note the PPO around the collar of the uHead prosthesis (white arrows) and the impingement between the radial ReMotion component and the distal part of scaphoid after standard horizontal resection (yellow arrow, A3). (B1-2): Intraoperative dynamic fluoroscopy of a ReMotion implant (sagittal plane) demonstrating a possible passive flexion of 50° after all, note that the offset of the exactly aligned radial component is perpendicular to the longitudinal axis of radius shaft (i.e. no volar tilt like in a normal wrist) and the carpal component is exactly aligned to the 3rd metacarpal-capitate axis as well (yellow pointed and blue lines) (B1). Same patient at the 1-year follow-up, the active flexion is marked decreased to 15° only (B2).
{kind=link}
In decision making TWR vs. TWA the patient’s expectations and experiences must be considered. Larsson et al. [26] found that living with unbearable constant pain and the desire to be free from it is the breakpoint for the patients to undergo extensive wrist surgery, and patients who had either a TWR or a TWA as a first-line treatment experienced more pain relief after surgery than patients who had undergone several previous wrist surgeries, therefore, surgeons might address the discussion about having one of both procedures earlier in the therapeutic management. Additionally, longstanding impaired wrist motion prior to TWA is associated with a better outcome after surgery than in patients with a short time of duration [26]. Furthermore, positive or negative thinking by the patients may have influence on their outcome after TWR or TWA, and this can be positively influenced by the surgeons giving accurate informations about the advantages and disadvantages of both procedures before surgery so that patients also feel like patients without medical knowledge and not like colleagues of the surgeon [26]. Interestingly, in this study some patients undergoing TWA reported that the alternative of a TWR was never discussed before surgery suggesting that could be based on insufficiently available knowledge about recent evidence, personal experience and technical skills by the surgeons [26].
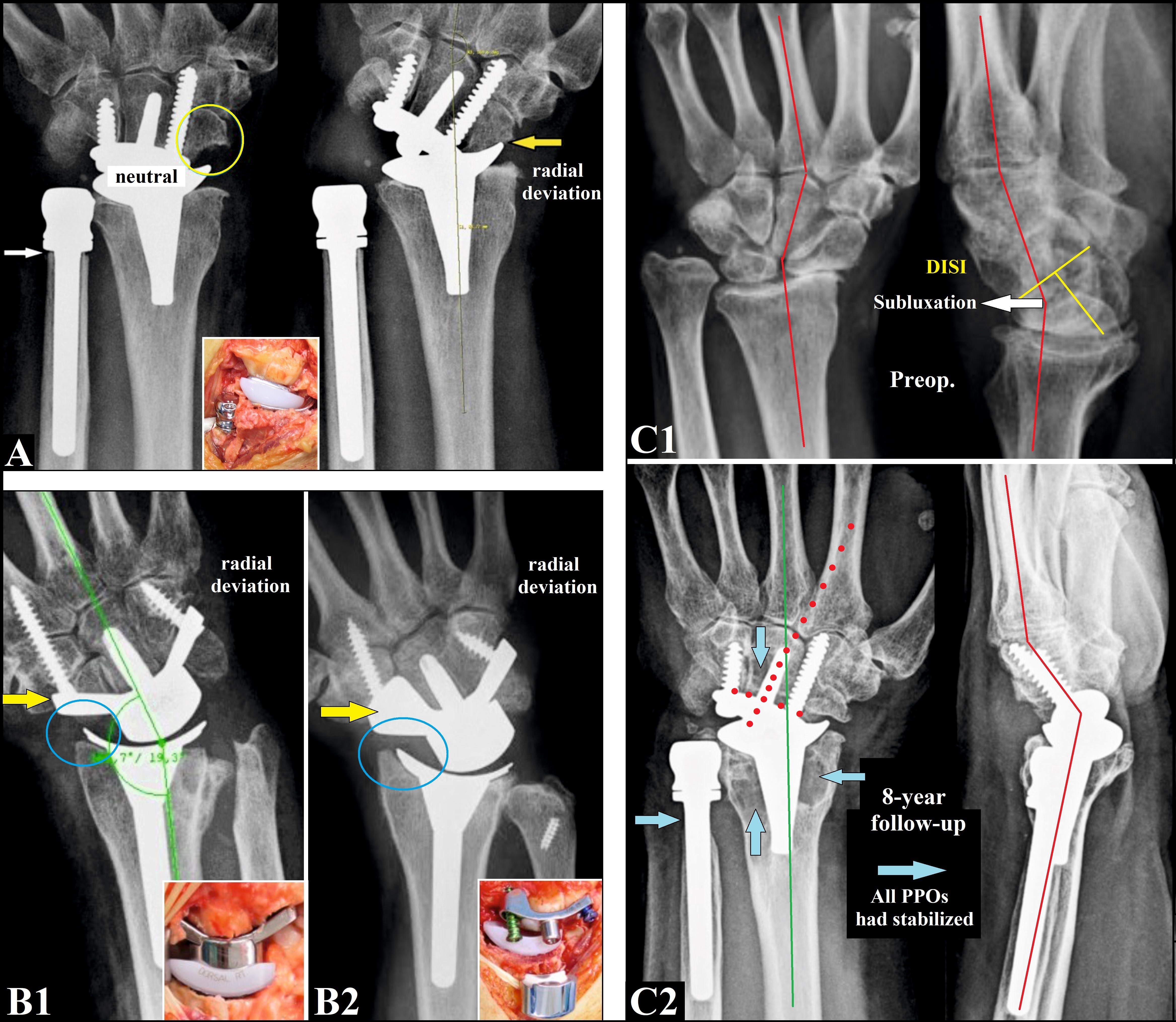
[14]: (A) This 59-year-old female presented with left distal radius physeal arrest after a DRF with age of 11 years received primary combined replacements. The uHead prosthesis was pressfit inserted on the top of the distal ulnar stump (white arrow). Despite additional diagonal resection at the scaphoid a painful impingement between the radial ReMotion component (cementless) and the sacphoid with terminal range of radial deviation was observed (yellow arrow). Note the straight horizontal design of the carpal component. (B1-2) The radiograph of a 1st Maestro type (without a scaphoid augment, yellow arrow) showing no impingement with terminal range of radial deviation (yellow blue circle, B1), same situation with a 2nd Maestro type with scaphoid augment, note the concave to distally curved design of the carpal components for both types (B2). (C1-2) Same patient as in (A), the preoperative radiographs showing advanced stage of post-traumatic arthritis due to a pronounced carpal malalignment (Z-deformity, red lines) with marked dorsal intercalated segment instability (yellow lines) followed by fixed subluxation of the capitate against the lunate in dorsal direction (white arrow, C1). At the 8-year follow up, all PPOs had stabilized (steady state, yellow blue arrows). Note that the Z-deformity could be corrected in the frontal plane only by an incorrectly aligned carpal plate (green and red pointed lines, compromise solution) but not in the sagittal plane (red lines). The patient is unchanged pain free and very satisfied with her outcome, however, the persistent deformity must be considered as potential risc factor for mechanical failure of the carpal component (C2). This case was formerly published in 2014 at a 1-year follow-up [7]. Supplementary material: Videos 5 and 6 demonstrate well functioning circumduction and „dart thrower’s“ motion at the 9-year follow-up.
{kind=link}
Outcomes and problems of TWR
Rheumatoid arthritis is the most common etiology of patients receiving TWR (71%), followed by post-traumatic conditions with 14% (scapholunate advanced collapse (SLAC) 6%, scapho-nonunion advanced collapse (SNAC) 4%, other 4%), other degenerative causes with 4%, Kienböck’s disease with 2%, and 9% with not well specified causes [6]. Between 2001 and 2013 1,201 patients received a TWR in USA (National Inpatient Sample Database, ICD-9 code 81.73) with a female predominance (71%), 51.5% of them were aged 60+ years and followed by 25.0% in patients aged 50-59 years, and the majority of procedures (60.8%) were performed at urban teaching hospitals often regarded as academic centers of excellence, but the total numbers of procedures decreased by 26% annually [48]. The statistically significant decrease in frequency of arthroplasties (23%), arthrodeses (18%) as well as synovectomy procedures (39%) in particular in rheumatic patients was confirmed by a study from UK involving a total number of 1,109 wrist procedures (female to male ratio 4.9:1) between 1996 and 2009, and this is based on the effectiveness of the modern anti-rheumatic drugs, noted that only the total number of tendon surgery (21%) did not decrease significantly [49].
(primarily published in [76], Copyright Ingo Schmidt): (A) A 39-year-old male presented with a left fracture-dislocation injury after a fall from height. (B) Primary treatment by open reduction and internal fixation (dorsal and volar plating). (C) One year after injury, a ponounced post-traumatic arthritis developed, both plates were removed, note the primarily overlooked scapholunate dissociation (yellow arrow). (D) Intraoperative fluoroscopy and clinical photographs showing the correctly inserted ReMotion implant after removal of the entire scaphoid (yellow arrow), cement augmentation of the not bony wrapped proximal part of the radial-sided fixation screw, and no impingement with terminal range of radial deviation (yellow blue circle and lines). (D) At the 1-year follow-up there was unchanged correct positioning of the ReMotion. Despite the marked decreased flexion compared to the right unaffected wrist the patient could be re-employed in his high-demand occupation as a mechanic. Supplementary material: Videos 7 and 8 demonstrate well functioning circumduction at the 2-year follow-up whereas „dart thrower’s“ motion is deteriorated towards to flexion-ulnar deviation but not towards to extension-radial deviation that is based on the overal marked decreased flexion and ulnar deviation.
{kind=link}
No reliable data exist on how a TWR can be exposed in vivo to maximum of load over a long time, therefore, in order to avoid PE wear and/or fracture, the mean age of patients who underwent a TWR with 58.3 years differs unchanged significantly to 52 years of patients who underwent a TWA (p < 0.001) [27]. Weiss and Akelman [50] advised their patients not to lift greater than 10 pounds in the hand which contains the total wrist implant from a safety perspective. However, there is a trend in the literature with encouraging results for detecting TWR in high-demand males with post-traumatic PPOA aged 52 years and younger if it exclusively wished by the patients and who are willing to accept the somewhat greater risk of revision surgery in the further course (Figure 7, Supplementary material: Videos 1-3) [51,52]. For this purpose, the use of dynamic or static orthotic devices imitating TWA during high-loaded occupational work can increase safety (Supplementary material: Video 4) [53, 54].
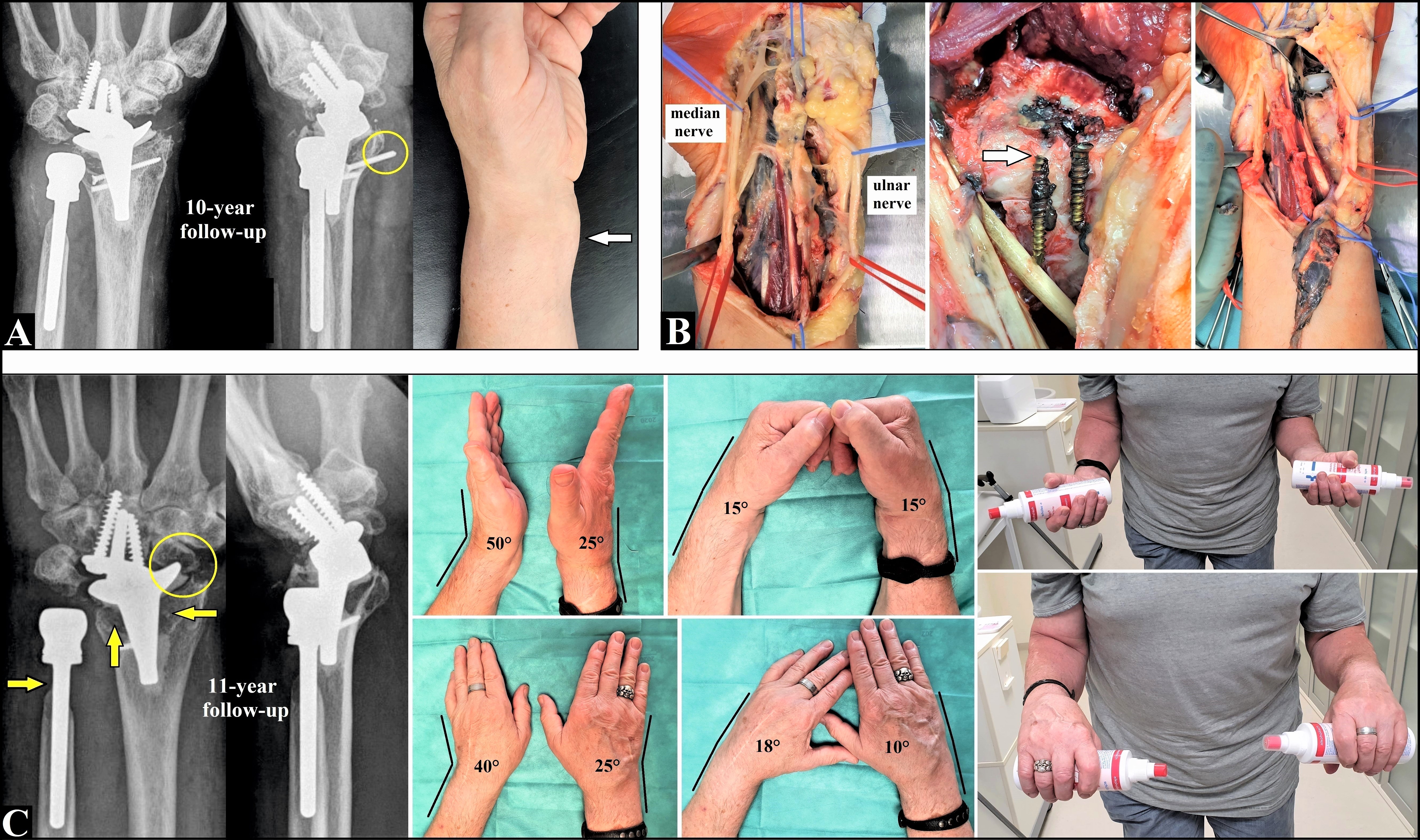
8 (Same patient as in Figures 5A1-3, now the 10-year follow-up, primarily published in [76], Copyright Ingo Schmidt): (A) Migration of one screw to volar (yellow circle), painful swelling at the volar aspect of the wrist (white arrow), both ReMotion components are not loosened. (B) Massive metallosis originating from the holes of the non-locking fixation screws of the carpal component, the two 3.5 mm titanium compression screws were loosened within the PPO and one of them was broken (white arrow, this screw head could not be removed), a radical soft tissue debridement was done. (C) One year after revision there was no recurrence of metallosis. Both ReMotion components are unchanged not loosened, note the stabilized PPO around all implants (yellow arrows) and the marked radial impingement that led to a erosion into the scaphoid (yellow circle). The patient is unchanged pain free and very satisfied with his functional outcome. Supplementary material: Video 9 demonstrates well functioning circumduction at the 11-year follow-up.
{kind=link}
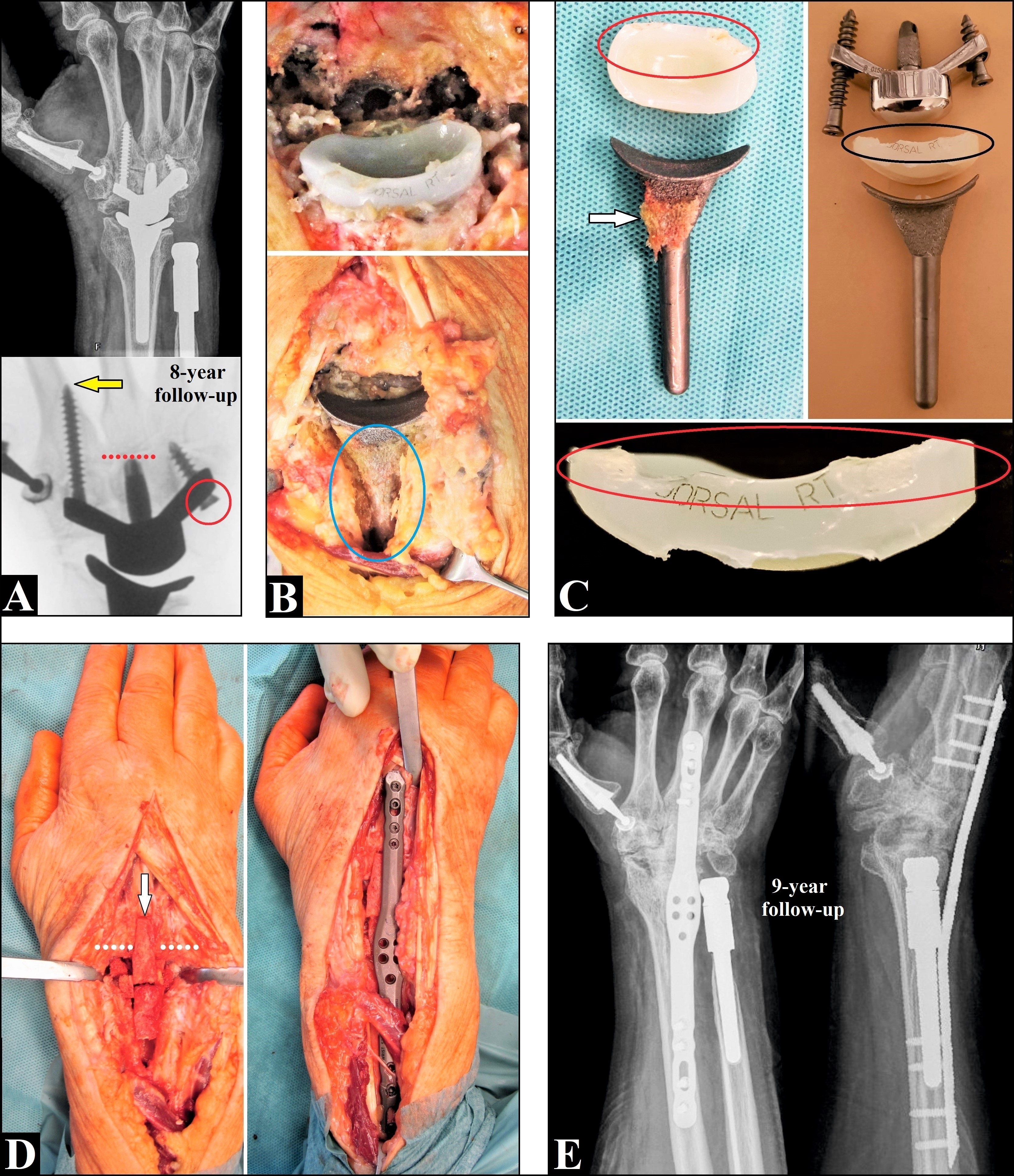
(Same patient as in Figure 2, now the 8-year follow-up [14]): (A) Both non-locking screws were loosened and the ulnar-sided was dislocated into the articular space (red arrow). The carpal component was subsided (red pointed line, in comparison to the yellow pointed lines in Figure 2) accompanied by cortical migration of the radial-sided screw (yellow arrow). Therefore, the conversion to a TWA became neccessary. (B) Intraoperatively, metallosis was present originating from the holes of both loosened screws and the capitate peg. For removal of the well osseointegrated radial component with it porous titanium coated radial body a large bony windowing at the dorsal aspect of the distal radius was required (blue oval circle). (C) Photographs of the explanted 1st Maestro type showing the well osseointgrated radial component (white arrow) and considerable PE abrasions at the dorsal edge of the insert (oval circles). The explant analysis revealed that the explant was found to operate under boundary lubrication associated with oxidation areas mainly in the centre of the insert [58]. (D) The TWA was done utilizing two corticocancellous iliac crest bone grafts (white arrow) crossing the CMCJ III (white pointed lines) into the 3rd metacarpal, and a 3.5/2.7 mm titanium wrist spanning plate. (E) One year after TWA there was a uneventful bony fusion, and the other two implants (Arpe, uHead) unchanged are well functioning.
{kind=link}
Regarding the design there are some differences between the 3rd generation types. Both the Universal2/Freedom and the ReMotion work with an intercalated PE ball articulating in a metal cup of the radial components whereas the Maestro is (was) similiar to a small total hip replacement in which the distal metal head articulates in a proximal PE cup. However, the disadvantage of the Maestro is (was) that the PE insert is fixed to the radial body, and in case of PE problems the entire radial component had to be removed and/or exchanged requiring a large bony windowing although it is well osseointegrated with its porous titanium coated radial body (Figure 9B/C). An adjustment of the Maestro was made with the introduce of its 2nd type, for an exchange of the intercalated metal head the entire carpal plate no longer needed to be replaced (Figure 3).
(51-year-old female, complicated course of a giant cell tumor at the right capitate, formerly published at a 1-year follow-up [9], now the 5-year follow-up [14]): (A) Around the entire stem of radial component (2nd Maestro type, cementless) marked radiolucencies are present (yellow arrows) associated with asymptomatic subsidence (yellow line). There is a complete osteonecrosis around the entire capitate peg (yellow oval circle), but both locking screws are not loosened, and the carpal component is not subsided. (B) The patient is unchanged pain free and very satisfied with her functional outcome. Supplementary material: Videos 10 and 11 demonstrate well functioning circumduction and „dart thrower’s“ motion at the 6-year follow-up.
{kind=link}
Regarding survivorship (8 to 15 years) the Maestro is (was) with 95% superior over the ReMotion (90%) and the Universal2 (78%), and that can considered to be as result with the use of the 2nd Maestro type with locking screws for fixation of the carpal component in contrast to the ReMotion as well as the Universal2 (Figures 1, 3-10) [29, 44, 55-58]. These results are absolutely comparable (or better) to those after total shoulder, elbow, and ankle replacements which are less debate in the literature. It remains to be seen whether recent reported encouraging short-term results with the Freedom (now with locking screws too) will be superior in mid- to long-term survivorship over the Universal2 [59]. Noted that the author of this article content has contacted the companies offering the ReMotion several times (stryker and Small Bone Innovations (USA) prior to stryker) to equip this implant with locking screws as well (and also with an additional 3rd larger intercalated PE ball for a better restoration of the resection-related loss of carpal height), but all requests remained unanswered.
The following outcomes are based on data extracted from three systematic review articles, and noted that for Patient-reported outcome measures (PROMs) the DASH and PRWE both have evidence of reliability, validity, and responsiveness for wrist pathologies [29, 60-62]: Both TWR including all 3rd generation types and TWA are effective in reducing pain and improvement in DASH, and a poorer outcome in pain relief after TWR correlates with a poorer DASH. The DASH in patients with a TWR due to non-inflammatory disease is accompanied by a significantly better improvement than in patients with inflammatory disease (p = 0.005), but in QuickDASH no differences were found between rheumatic and non-rheumatic patients. The mean improvement in grip strength for TWR is 19% compared to preop., and no relevant differences were found compared to the unaffected contralateral wrist between TWR (58 – 72%) and TWA (50 – 79%). One study each revealed a return to work in 100% of patients with the Universal2 and 83% with the ReMotion, and no valid data exist about with the use of the Maestro but it was reported in a single case on a 31-year-old male with high claims in work and leisure [52]. Noted that a return to work in younger patients (average age 41 years, range 24-63) received a first-line TWA is achieved in 65% of cases only [17].
The functional outcome shows substantial differences between the implants with the Maestro being significantly superior to both the Universal2 and ReMotion in summation, and the following data were extracted from seven studies with a total number of 334 patients (mean differences pre- to postop.) [15]: (1) extension is improved for all implants (Universal2 +7.6°, ReMotion +5.8°, Maestro +16°), (2) flexion is equal with the Universal2 and detoriated for both the ReMotion (-4.1°) and the Maestro (-6°) (Figures 3, 5B1/2 and 7), (3) ulnar deviation is improved for all implants (Universal2 +3.5°, ReMotion +4.1°, Maestro +11°), and (4) radial deviation is deteriorated for both the Universal2 (-4.1°) and ReMotion (-1.8°) whereas improved only with the Maestro (+5.5°). Both biological and design-related issues must be considered as reasons for the deterioration of flexion for all implants: (1) scarring around the large dorsal incision accompanied by loss of elasticity of the wrist capsule [3], and (2) the radial components of all implants with its straight offsets perpendicular to the longitudinal axis of the radius shaft do not obtain the anatomical volar tilt of the articular surface in the sagittal plane (Figure 5B1) [14, 63]. The deterioration of wrist motion in opposite direction to the surgical incision due to scarring of the wrist capsule is a concern and also known from surgery of dorsal or volar wrist ganglions, and volar plating for treatment of DRF [64-66]. With regard to the known biomechanical findings about coupled wrist motion in TWR, the expected restriction of circumduction as well as the „dart-thrower’s“ motion is clinically often only of secondary relevance with our patients, and if slightly deteriorated, mostly not perceived as impaired by them (Supplementary material: Videos 1, 5-7, 9-11). But noted that an overall deteriorated flexion may have negative influence for „dart thrower’s“ motion towards to flexion-ulnar deviation alone (Supplementary material: Video 8). The rationale behind our clinical observation is that for performing the most important and frequent ADL only or less than 60% of the total wrist motion capacity is required, and, in contrast as prior assumed, the radiocarpal joint seems to be able to compensate the „dart thrower’s“ motion if the midcarpal joint is locked [21, 67]. Additionally, the intercalated carpal ball of the ReMotion can rotate 10° relative to the carpal component providing equivalent midcarpal joint motion as mentioned by the developer (Supplementary material: Video 12) [68].
The deteriorated radial deviation with the ReMotion manifests itself clinically with a painful radial impingement between the offset of the radial component and the scaphoid in both for the standard straight horizontal resection and an additional diagonal resection potentially leading to bony erosions into the distal part of scaphoid, and this can be avoided with removal of the entire scaphoid only (Figures 5A3, 6A, 7D and 8C) [7, 69]. Painful radial impingement is also observed after proximal row carpectomy, therefore, the ReMotion with it only available two intercalated PE balls is obviously not able to restore completely the resection-related loss of carpal height [15]. Noted that this impingement is often only detectable radiographically with the use of dynamic radiographs (terminal range of radial deviation) and not with a wrist held in static neutral position (Figure 6A). However, when the entire scaphoid is removed then the proximal part of the radial-sided fixation screw is not bony wrapped, and this must be considered as potential risk factor for mechanical failure. Froschauer et al. [70] reported about encouraging results with 21 patients (22 wrists) received a TWR with the ReMotion primarily combined with proximal row carpectomy and radial styloid resection, and at a mean time follow-up of 5.5 years radial deviation had improved from 10° to 15° (postop.) but there were still three special complications (13.7%, one case with subsidence of the carpal plate / two cases with screw breakages). With regard to this follow-up, it must be noted that the survivorship of all 3rd generation types is 90 - 100% at 5 years in most series, but it declines from 5 to 8 years [6]. Noted as well that a radial styloid resection should be performed only distal to the origin of the radioscaphocapitate ligament (i.e. level A) to avoid instability of the wrist presented as radial wrist pain and/or ulnar carpal (prosthetic) dislocation tendency [52, 71, 72]. A novel approach in order to enhance the stability of the radial-sided screw could be cement augmentation of it. The background of this modified concept is the improvement of its pullout strength that has been prior well established for use at the spine, and for treatment of proximal humeral as well as intertrochanteric femoral fractures in the elderly [73-75]. For TWR only in a single case report at a short-term follow-up was reported about that in the literature („off label“ use), and further studies are needed to validate this concept (Figure 7) [76]. If the deteriorated radial deviation with the Universal2 / Freedom is also accompanied by a painful radial impingement is unknown to the author of this article content. The improvement of radial deviation with the Maestro is (was) considered to be as design-related advantage. In contrast to the ReMotion with it straight horizontal offset of the carpal component (also with the Univeral2 and Freedom), the offset of the Maestro is (was) concave to distally curved and the option for use of three intercalated metal heads allows a better restoration of the resection-related loss of carpal height (Figure 6).
Despite the superiority of the Maestro in terms of design with it high modularity, survivorship and functional outcome over the other types, this implant was surprisingly withdrawn from the marketplace by the company in February 2018 before the upcoming new CE certification worldwide. Zimmer Biomet stated officially that the Maestro was approved only for its cemented use by the US Food and Drug Administration and there were no publications in the literature about favorable results with it cemented use, and so, it cannot be guaranteed the surveillance of this implant if it inserted in a cementless manner (i.e. „off label“ use). This statement is incomprehensible and contradicts any scientific knowledge. All 3rd generation types have porous titanium coated radial stems in order to induce a sufficient osseointegration (Figure 9B/C) which is absolutely comparable with all modern total hip replacements. There is a consensus in the literature that primary cementation is detected only in cases with poor osteoporotic or rheumatoid-related bone stock, periprosthetic fractures, revision TWR, and for the use of custom-made implants for treatment of large tumors at the distal radial metaphysis such the giant cell tumor (Figures 1 A/B and 4) [1, 2, 5, 6, 10, 13, 44, 77]. Moreover, a sufficient cementation of the carpal components with all 3rd generation TWR types is factually not possible. The cement placed into the small drilled holes would inevitably squeezed out when the capitate peg and the fixation screws are inserted. And now all surgeons have explanation miseries to their patients if a Maestro has been failed (a question to the author of this book chapter by a patient of him: „Doctor, why did I get a bad prosthesis implanted?“). For those cases the conversion to TWA is probably the only salvage option of choice [43]. Due to the required design-related deep metaphyseal insertion of the radial body with the Maestro, a motion-preserving revision TWR utilizing the ReMotion or Freedom with its shorter radial stems without the opportunity for a pressfit insertion into the diaphysis appears to be impossible or at least very questionable by a supporting filling off the deep cavity with cement. Interestingly, Zimmer Biomet offers unchanged the Taperloc hip prosthesis for use only in a cementless manner, and this prosthesis with it porous titanium coated trochanteric part has an absolutely comparable stem design for osseintegration like the Maestro [78]. Therefore, it must be suggested that the Maestro was no longer profitable for the company [43, 44, 79].
Failure of TWR and salvage options
Rheumatoid arthritis is the most common etiology of patients receiving TWR (71%), followed by post-traumatic conditions with 14% (scapholunate advanced collapse (SLAC) 6%, scapho-nonunion advanced collapse (SNAC) 4%, other 4%), other degenerative causes with 4%, Kienböck’s disease with 2%, and 9% with not well specified causes [6]. Between 2001 and 2013 1,201 patients received a TWR in USA (National Inpatient Sample Database, ICD-9 code 81.73) with a female predominance (71%), 51.5% of them were aged 60+ years and followed by 25.0% in patients aged 50-59 years, and the majority of procedures (60.8%) were performed at urban teaching hospitals often regarded as academic centers of excellence, but the total numbers of procedures decreased by 26% annually [48]. The statistically significant decrease in frequency of arthroplasties (23%), arthrodeses (18%) as well as synovectomy procedures (39%) in particular in rheumatic patients was confirmed by a study from UK involving a total number of 1,109 wrist procedures (female to male ratio 4.9:1) between 1996 and 2009, and this is based on the effectiveness of the modern anti-rheumatic drugs, noted that only the total number of tendon surgery (21%) did not decrease significantly [49].
No reliable data exist on how a TWR can be exposed in vivo to maximum of load over a long time, therefore, in order to avoid PE wear and/or fracture, the mean age of patients who underwent a TWR with 58.3 years differs unchanged significantly to 52 years of patients who underwent a TWA (p < 0.001) [27]. Weiss and Akelman [50] advised their patients not to lift greater than 10 pounds in the hand which contains the total wrist implant from a safety perspective. However, there is a trend in the literature with encouraging results for detecting TWR in high-demand males with post-traumatic PPOA aged 52 years and younger if it exclusively wished by the patients and who are willing to accept the somewhat greater risk of revision surgery in the further course (Figure 7, Supplementary material: Videos 1-3) [51,52]. For this purpose, the use of dynamic or static orthotic devices imitating TWA during high-loaded occupational work can increase safety (Supplementary material: Video 4) [53, 54].
Regarding the design there are some differences between the 3rd generation types. Both the Universal2/Freedom and the ReMotion work with an intercalated PE ball articulating in a metal cup of the radial components whereas the Maestro is (was) similiar to a small total hip replacement in which the distal metal head articulates in a proximal PE cup. However, the disadvantage of the Maestro is (was) that the PE insert is fixed to the radial body, and in case of PE problems the entire radial component had to be removed and/or exchanged requiring a large bony windowing although it is well osseointegrated with its porous titanium coated radial body (Figure 9B/C). An adjustment of the Maestro was made with the introduce of its 2nd type, for an exchange of the intercalated metal head the entire carpal plate no longer needed to be replaced (Figure 3).
Regarding survivorship (8 to 15 years) the Maestro is (was) with 95% superior over the ReMotion (90%) and the Universal2 (78%), and that can considered to be as result with the use of the 2nd Maestro type with locking screws for fixation of the carpal component in contrast to the ReMotion as well as the Universal2 (Figures 1, 3-10) [29, 44, 55-58]. These results are absolutely comparable (or better) to those after total shoulder, elbow, and ankle replacements which are less debate in the literature. It remains to be seen whether recent reported encouraging short-term results with the Freedom (now with locking screws too) will be superior in mid- to long-term survivorship over the Universal2 [59]. Noted that the author of this article content has contacted the companies offering the ReMotion several times (stryker and Small Bone Innovations (USA) prior to stryker) to equip this implant with locking screws as well (and also with an additional 3rd larger intercalated PE ball for a better restoration of the resection-related loss of carpal height), but all requests remained unanswered.
The following outcomes are based on data extracted from three systematic review articles, and noted that for Patient-reported outcome measures (PROMs) the DASH and PRWE both have evidence of reliability, validity, and responsiveness for wrist pathologies [29, 60-62]: Both TWR including all 3rd generation types and TWA are effective in reducing pain and improvement in DASH, and a poorer outcome in pain relief after TWR correlates with a poorer DASH. The DASH in patients with a TWR due to non-inflammatory disease is accompanied by a significantly better improvement than in patients with inflammatory disease (p = 0.005), but in QuickDASH no differences were found between rheumatic and non-rheumatic patients. The mean improvement in grip strength for TWR is 19% compared to preop., and no relevant differences were found compared to the unaffected contralateral wrist between TWR (58 – 72%) and TWA (50 – 79%). One study each revealed a return to work in 100% of patients with the Universal2 and 83% with the ReMotion, and no valid data exist about with the use of the Maestro but it was reported in a single case on a 31-year-old male with high claims in work and leisure [52]. Noted that a return to work in younger patients (average age 41 years, range 24-63) received a first-line TWA is achieved in 65% of cases only [17].
The functional outcome shows substantial differences between the implants with the Maestro being significantly superior to both the Universal2 and ReMotion in summation, and the following data were extracted from seven studies with a total number of 334 patients (mean differences pre- to postop.) [15]: (1) extension is improved for all implants (Universal2 +7.6°, ReMotion +5.8°, Maestro +16°), (2) flexion is equal with the Universal2 and detoriated for both the ReMotion (-4.1°) and the Maestro (-6°) (Figures 3, 5B1/2 and 7), (3) ulnar deviation is improved for all implants (Universal2 +3.5°, ReMotion +4.1°, Maestro +11°), and (4) radial deviation is deteriorated for both the Universal2 (-4.1°) and ReMotion (-1.8°) whereas improved only with the Maestro (+5.5°). Both biological and design-related issues must be considered as reasons for the deterioration of flexion for all implants: (1) scarring around the large dorsal incision accompanied by loss of elasticity of the wrist capsule [3], and (2) the radial components of all implants with its straight offsets perpendicular to the longitudinal axis of the radius shaft do not obtain the anatomical volar tilt of the articular surface in the sagittal plane (Figure 5B1) [14, 63]. The deterioration of wrist motion in opposite direction to the surgical incision due to scarring of the wrist capsule is a concern and also known from surgery of dorsal or volar wrist ganglions, and volar plating for treatment of DRF [64-66]. With regard to the known biomechanical findings about coupled wrist motion in TWR, the expected restriction of circumduction as well as the „dart-thrower’s“ motion is clinically often only of secondary relevance with our patients, and if slightly deteriorated, mostly not perceived as impaired by them (Supplementary material: Videos 1, 5-7, 9-11). But noted that an overall deteriorated flexion may have negative influence for „dart thrower’s“ motion towards to flexion-ulnar deviation alone (Supplementary material: Video 8). The rationale behind our clinical observation is that for performing the most important and frequent ADL only or less than 60% of the total wrist motion capacity is required, and, in contrast as prior assumed, the radiocarpal joint seems to be able to compensate the „dart thrower’s“ motion if the midcarpal joint is locked [21, 67]. Additionally, the intercalated carpal ball of the ReMotion can rotate 10° relative to the carpal component providing equivalent midcarpal joint motion as mentioned by the developer (Supplementary material: Video 12) [68].
The deteriorated radial deviation with the ReMotion manifests itself clinically with a painful radial impingement between the offset of the radial component and the scaphoid in both for the standard straight horizontal resection and an additional diagonal resection potentially leading to bony erosions into the distal part of scaphoid, and this can be avoided with removal of the entire scaphoid only (Figures 5A3, 6A, 7D and 8C) [7, 69]. Painful radial impingement is also observed after proximal row carpectomy, therefore, the ReMotion with it only available two intercalated PE balls is obviously not able to restore completely the resection-related loss of carpal height [15]. Noted that this impingement is often only detectable radiographically with the use of dynamic radiographs (terminal range of radial deviation) and not with a wrist held in static neutral position (Figure 6A). However, when the entire scaphoid is removed then the proximal part of the radial-sided fixation screw is not bony wrapped, and this must be considered as potential risk factor for mechanical failure. Froschauer et al. [70] reported about encouraging results with 21 patients (22 wrists) received a TWR with the ReMotion primarily combined with proximal row carpectomy and radial styloid resection, and at a mean time follow-up of 5.5 years radial deviation had improved from 10° to 15° (postop.) but there were still three special complications (13.7%, one case with subsidence of the carpal plate / two cases with screw breakages). With regard to this follow-up, it must be noted that the survivorship of all 3rd generation types is 90 - 100% at 5 years in most series, but it declines from 5 to 8 years [6]. Noted as well that a radial styloid resection should be performed only distal to the origin of the radioscaphocapitate ligament (i.e. level A) to avoid instability of the wrist presented as radial wrist pain and/or ulnar carpal (prosthetic) dislocation tendency [52, 71, 72]. A novel approach in order to enhance the stability of the radial-sided screw could be cement augmentation of it. The background of this modified concept is the improvement of its pullout strength that has been prior well established for use at the spine, and for treatment of proximal humeral as well as intertrochanteric femoral fractures in the elderly [73-75]. For TWR only in a single case report at a short-term follow-up was reported about that in the literature („off label“ use), and further studies are needed to validate this concept (Figure 7) [76]. If the deteriorated radial deviation with the Universal2 / Freedom is also accompanied by a painful radial impingement is unknown to the author of this article content. The improvement of radial deviation with the Maestro is (was) considered to be as design-related advantage. In contrast to the ReMotion with it straight horizontal offset of the carpal component (also with the Univeral2 and Freedom), the offset of the Maestro is (was) concave to distally curved and the option for use of three intercalated metal heads allows a better restoration of the resection-related loss of carpal height (Figure 6).
Despite the superiority of the Maestro in terms of design with it high modularity, survivorship and functional outcome over the other types, this implant was surprisingly withdrawn from the marketplace by the company in February 2018 before the upcoming new CE certification worldwide. Zimmer Biomet stated officially that the Maestro was approved only for its cemented use by the US Food and Drug Administration and there were no publications in the literature about favorable results with it cemented use, and so, it cannot be guaranteed the surveillance of this implant if it inserted in a cementless manner (i.e. „off label“ use). This statement is incomprehensible and contradicts any scientific knowledge. All 3rd generation types have porous titanium coated radial stems in order to induce a sufficient osseointegration (Figure 9B/C) which is absolutely comparable with all modern total hip replacements. There is a consensus in the literature that primary cementation is detected only in cases with poor osteoporotic or rheumatoid-related bone stock, periprosthetic fractures, revision TWR, and for the use of custom-made implants for treatment of large tumors at the distal radial metaphysis such the giant cell tumor (Figures 1 A/B and 4) [1, 2, 5, 6, 10, 13, 44, 77]. Moreover, a sufficient cementation of the carpal components with all 3rd generation TWR types is factually not possible. The cement placed into the small drilled holes would inevitably squeezed out when the capitate peg and the fixation screws are inserted. And now all surgeons have explanation miseries to their patients if a Maestro has been failed (a question to the author of this book chapter by a patient of him: „Doctor, why did I get a bad prosthesis implanted?“). For those cases the conversion to TWA is probably the only salvage option of choice [43]. Due to the required design-related deep metaphyseal insertion of the radial body with the Maestro, a motion-preserving revision TWR utilizing the ReMotion or Freedom with its shorter radial stems without the opportunity for a pressfit insertion into the diaphysis appears to be impossible or at least very questionable by a supporting filling off the deep cavity with cement. Interestingly, Zimmer Biomet offers unchanged the Taperloc hip prosthesis for use only in a cementless manner, and this prosthesis with it porous titanium coated trochanteric part has an absolutely comparable stem design for osseintegration like the Maestro [78]. Therefore, it must be suggested that the Maestro was no longer profitable for the company [43, 44, 79].
Other designs and further developments
Another implant which is currently used is the Motec. The hemispherical ball-and-socket articulation either by a metal-on-metal or by a metal-on-polyetheretherketone (PEEK) gliding replicates both anatomical centers of rotation allocated at the proximal part of the capitate, and it can be considered a modified revival of older TWR types. First mid- to long-term results at a mean 8-year follow-up in high-demand patients with a mean age of 52 years (70.2% male) revealed promising results with a survival rate of 82% [51]. Both components with its conical straight stems are screwed deeply into the diaphyses that makes this implant also interesting for revision of a failed 3rd generation TWR with it shorter stems for both components. To minimize the risk of a dorsal breakthrough of the metacarpal stem as reported in one case, which was one of the major concern with the Biax as well, it is recommended to lift the capitate in dorsal direction exactly along the straight 3rd metacarpal-capitate line by performing a dorsal-wedged shaped resection combined with a fusion of the CMCJ III [36,37,105,106]. As further complications were reported about pseudotumor based on metallosis by using the metal-on-metal gliding, extensive synovitis based on adverse wear conditions in the cup by using the metal-on-PEEK gliding, and mechanical abrasions at the dorsal aspect of the hemispherical cup due to an impingement with the collar of the intercalated head component [107]. However, occurrence of dorsal impingement with the Motec can be avoided by inserting a longer intercalated head component which underlines the importance of restoration the resection-related loss of carpal height as already written in advance in this article content about the 3rd generation types [106]. In cases of a metal-induced synovitis a conversion to a metal-on-PEEK gliding is reported to be one salvage option [108].
A new 3rd generation type was introduced in 2020 and revealed promising results at a minimum 5-year follow-up with a survival rate of 100% in 20 patients that includes asymptomatic radiographic signs of loosening of the carpal components in five patients (26%) without the need of surgical revision [97]. Interestingly again, PPO occurred in only one of these cases at the final follow-up, whereas the other four cases were observed within 1.5 years after surgery and it had been stabilized after that. This type has similarities with the Maestro in which a distal convex metal head articulates in a proximal concave PE cup, and it has three additional features: (1) the flexion-extension axis is aligned to the midcarpal joint line in an effort to limit stress on surrounding soft tissues as stated by the authors, (2) the carpal component is supported by a volar flange (i.e. similar to the Coonrad/Morrey prosthesis for total elbow replacement) in an effort to resist the posterior and rotational displacement forces as stated by the authors as well, and (3) this implant is detected only for patients with poor osteoporotic or rheumatoid bone stock because the radial component consists of a PE monobloc for exclusive use in a cemented manner [97, 109]. The latter could prove problematic, if longstanding symptomatic surface PE wear or fracture occurs then the entire component must be revised even it may not be loosened, and noted that this was a worth considering disadvantage of the Biax as well as the Maestro and often possible only by a large bony windowing at the dorsal aspect of the distal radius meta-/diaphysis (Figure 9B) [37,58,110]. Therefore, removal of a cemented radial TWR component is certainly not entirely unproblematic, and in summary, any advantage of this specific radial PE monobloc component over the established porous titanium coated radial stems of the other 3rd generation types is not clearly discernible. Moreover, the problem of deteriorated flexion postoperatively observed in all other types is unchanged unsolved with this new type, and probably also based in its design with a likewise 90° bend of the offset of the radial component to its radial stem respectively radius shaft axis [97, 109].
Hooke et al. [31] reported about first biomechanical investigations with a new 3rd generation type which has similarities with the Maestro too and which could be able to improve circumduction as well as the “dart thrower’s” motion, but clinical data are not available currently. Another approach could be the development of a new type which replicates the anatomical volar tilt of the radial component in the sagittal plane to improve flexion postoperatively [62].
The 4th (or 5th) generation types either by radial hemiarthroplasty with an unphysiological “metal-on-cartilage gliding” or by proximal interposition or carpal hemiarthroplasty with the pyrocarbon implants were introduced to avoid mechanical failure of the carpal components in TWR [111,112]. The feature of the KinematX with it implant-specific replacement of the proximal row is the anatomically allocated preservation of both centers of rotation in midcarpal joint theoretically resulting in decreased mechanical stress onto the component and simultaneously improved coupled wrist motion in comparison to TWR [113,114]. Various other implants with or without replacement of the distal radius metaphysis (Sophia, Cobra, Isoelastic Resurfacing Prosthesis) are currently used for treatment of highly comminuted DRF in the elderly with the aim of an early reintegration of the patients in their social environment [115-118]. However, the limitation of the high-friction “metal-on-cartilage gliding” could be erosion into opposing bones known from the monopolar hemiarthroplasty at the hip and observed at the wrist in 6% of cases in the approved carpal hemiarthroplasty with the Maestro that was additionally complicated by painful dislocation tendency in ulnar direction due to a mismatch in size between the carpal prosthetic head and the lunate facet [119-121]. The outcome with use of the Maestro as radial hemi wrist implant (i.e. “cartilage-on-PE gliding”, “off label” use) revealed inacceptable high complication rates based on PE wear and resulting in pronounced tenosynovitis (“poly disease”) as well as bony erosions in 50% of cases [110,120]. In summary, it remains to be seen whether or not the 4th generation types will actually be superior over the established 3rd generation types in future.
Another novel designs such the KinematX total wrist (Extremity, USA; Figure 11) and the Anika (USA) as total or hemi wrist are in use, but clinical outcome data are currently not available.
(KinematX total wrist, Courtesy of Prof. Scott Wolfe, New York, USA, © 2022): (A) Intraoperative fluoroscopy with terminal range of radial and ulnar deviation showing no impingement. (B) Intraoperative fluoroscopy with terminal range of extension and flexion showing no impingement.
{kind=link}
Conclusion
TWR is a viable salvage procedure in treatment of PPOA and not only detected in the elderly. Regardless of this, all surgeons who are willing to start with it need a learning curve. The knowledge about recent evidence and features in design of the available types, exact assessment of radiographic findings, presence of technical skills by the surgeons, and observance of the patient's expectations are the basic requirements for a successful TWR.
Consent for publication
Not applicable
Conflict of interest
The author declares no conflict of interest, financial or otherwise.s.
Funding
None
Acknowlewdgements
Declared none.
References
Adams BD. Total wrist arthroplasty. Orthopedics. 2004;27(3):378-84.
Herzberg G. Total Wrist Arthroplasty: New Perspectives. Curr Rheumatol Rev. 2012;8(4):239-44.
Nydick JA, Greenberg SM, Stone JD, Williams B, Polikandriotis JA, Hess AV. Clinical outcomes of total wrist arthroplasty. J Hand Surg Am. 2012;37(8):1580-4.
Boeckstyns ME, Herzberg G, Merser S. Favorable results after total wrist arthroplasty: 65 wrists in 60 patients followed for 5-9 years. Acta Orthop. 2013;84(4):415-9.
Reigstad O, Røkkum M. Wrist arthroplasty: where do we stand today? A review of historic and contemporary designs. Hand Surg. 2014;19(2):311-22.
Boeckstyns ME. Wrist arthroplasty--a systematic review. Dan Med J. 2014;61(5):A4834.
Schmidt I. Primary combined replacements for treatment of distal radius physeal arrest. J Wrist Surg. 2014;3(3):203-5.
Schmidt I. Can Total Wrist Arthroplasty Be an Option for Treatment of Highly Comminuted Distal Radius Fracture in Selected Patients? Preliminary Experience with Two Cases. Case Rep Orthop. 2015;2015:380935.
Schmidt I. An Unusual and Complicated Course of a Giant Cell Tumor of the Capitate Bone. Case Rep Orthop. 2016;2016:370580.
Halim A, Weiss AC. Total Wrist Arthroplasty. J Hand Surg Am. 2017;42(3):198-209.
Schmidt I. Kienböck’s disease mimicing gouty monoarthritis of the wrist. Int J Case Rep Images. 2017;8(6):423-6.
Schmidt I. Distal radioulnar synostosis after primary combined replacements for treatment of highly comminuted distal radius fracture in an elderly patient. J Hand Surg Eur Vol. 2017;42(1):97-8.
Srnec JJ, Wagner ER, Rizzo M. Total Wrist Arthrpolasty. JBJS Rev. 2018;6(6):e9.
Schmidt I. Trendsetters for Total Wrist Arthroplasty: Ideas and Outcomes from Across the Pond. 77th Annual Meeting of the American Society for Surgery of the Hand (ASSH), Boston 2022 (Lecture, Symposium SYM11, 10/01/2022, https://www.researchgate.net/publication/360652747_Trendsetters_for_Total_Wrist_Arthroplasty_Ideas_and_Outcomes_From_Across_the_Pond_ASSH_Annual_Meeting_2022_Boston_SYM11_10012022)
Schmidt I. Functional Outcomes After Salvage Procedures for Wrist Trauma and Arthritis (Four-Corner Fusion, Proximal Row Carpectomy, Total Wrist Arthroplasty, Total Wrist Fusion, Wrist Denervation): A Review of Literature. Open Orthop J. 2019;13:217-31.
Adams BD, Grosland NM, Murphy DM, McCullough. Impact of impaired wrist motion on hand and upper-extremity performance (1). J Hand Surg Am. 2003;28(6):898-903.
Weiss AC, Wiedeman G Jr, Quenzer D, Hanington KR, Hastings H 2nd, Strickland JW. Upper extremity function after wrist arthrodesis. J Hand Surg Am. 1995;20(5):813-7.
Adey L, Ring R, Jupiter JB. Health status after total wrist arthrodesis for posttraumatic arthritis. J Hand Surg Am. 2005;30(5):932-6.
Ekroth SR, Werner FW, Palmer AK. Case report of long-term results of biaxial and volz total wrist arthroplasty. J Wrist Surg. 2012;1(2):177-8.
Nydick JA, Watt JF, Garcia MJ, Williams BD, Hess AV. Clinical outcomes of arthrodesis and arthroplasty for the treatment of posttraumatic wrist arthritis. J Hand Surg Am. 2013;38(5):899-903.
Nadeem M, Loss JG, Li ZM, Seitz Jr WH. Ulnar Extension Coupling in Functional Wrist Kinematics During Hand Activities of Daily Living. J Hand Surg Am. 2022;47(2):187.e1-187.e13.
Cantero-Téllez R, García Orza S, Bishop MD, Berjano P, Villafañe JH. Duration of wrist immobilization is associated with shoulder pain in patients with after wrist immobilization: an observational study. J Exerc Rehabil. 2018;14(4):694-8.
Schmidt I, Beylich T. A complicated course of extensor carpi ulnaris luxation. Trauma Emerg Care. 2020;5(3):203.
Jung HJ, Chang MJ, Kim KM, Yoo W, Jeon BJ, Hwang GC. Effect of Wrist Joint Restriction on Forearm and Shoulder Movement during Upper Extremity Functional Activities. J Phys Ther Sci. 2013;25(11):1411-4.
Gomes AD, Macedo Ricci FPF, Zampar AC, Pereira Santiago PR, de Cássia Registro Fonseca M. Influence of static wrist orthosis on muscle activity and shoulder and elbow range of motion during a functional task: a biomechanical study. Fisioter Pesqui. 2018;25(1):56-64.
Larsson S, Carlsson IK, Rosberg HE, Björkman A, Brogren E. Patients' experiences before and after total wrist fusion or total wrist arthroplasty:A qualitative study of patients with wrist osteoarthritis. J Hand Ther. 2022;35(1):41-50.
Melamed E, Marascalchi B, Hinds RM, Rizzo M, Capo JT. Trends in the Utilization of Total Wrist Arthroplasty versus Wrist Fusion for Treatment of Advanced Wrist Arthritis. J Wrist Surg. 2016;5(3):211-6.
Hinds RM, Capo JT, Rizzo M, Roberson JR, Gottschalk MB. Total Wrist Arthroplasty Versus Wrist Fusion; Utilization and Complication Rates as Reported by ABOS Part II Candidates. Hand (N Y). 2017;12(4):376-81.
Berber O, Garagnani L, Gidwani S. Systematic Review of Total Wrist Arthroplasty and Arthrodesis in Wrist Arthritis. J Wrist Surg. 2018;7(5):424-40.
Reigstad O, Holm-Glad T, Korslund J, Grimsgaard C, Thorkildsen R, Røkkum M. High re-operation and complication rates 11 years after arthrodesis of the wrist for non-inflammatory arthritis. Bone Joint J 2019;101-B(7):852-9.
Hooke AW, Pettersson K, Sagerfors M, An KN, Rizzo M. An anatomic and kinematic analysis of a new total wrist arthroplasty design. J Wrist Surg. 2015;4(2):121-7.
Singh HP, Bhattacharjee D, Dias JJ, Trail I. Dynamic assessment of the wrist after total wrist arthroplasty. J Hand Surg Eur Vol. 2017;42(6):573-9.
Akhbari B, Morton AM, Shah KN, et al. Proximal-distal shift of the center of rotation in a total wrist arthroplasty is more than twice of the healthy wrist. J Orthop Res. 2020;38(7):1575-86.
Akhbari B, Morton AM, Shah KN, et al. In vivo contact pattern of a total wrist arthroplasty design. J Biomech. 2021;121:110420.
Menon J. Universal Total Wrist Implant: experience with a carpal component fixed with three screws. J Arthroplasty. 1998;13(5):515-23.
Takwale VJ, Nuttall D, Trail IA, Stanley JK. Biaxial total wrist replacement in patients with rheumatoid arthritis. Clinical review, survivorship and radiological analysis. J Bone Joint Surg Br. 2002;84(5):692-9.
Kretschmer F, Fansa H. BIAX total wrist arthroplasty: management and results after 42 patients. Handchir Mikrochir Plast Chir. 2007;39(4):238-48.
Wolff J. Das Gesetz von der Transformation der Knochen. August Hirschwald: Berlin, 1892.
Schmidt I. Combined replacements using the Maestro total wrist and ulnar head implants. J Hand Surg Eur Vol. 2015;40(7):754-55.
Herren DB, Simmen BR. Limited and complete fusion of the rheumatoid wrist. J Am Soc Surg Hand. 2002;2(1):21-32.
de Roeck NJ, Packer GJ. Lunate migration following Darrach’s procedure. J Orthop Surg (Hong Kong). 2003;11(2):213-6.
Radmer S, Andresen R, Sparmann M. Total wrist arthroplasty in patients with rheumatoid arthritis. J Hand Surg Am. 2003;28(5):789-94.
Schmidt I. All surgeons who are planning a Total Wrist Arthroplasty with the MaestroTM implants should be aware. Recent Adv Arthroplast. 2018;2(2):69-74.
Schmidt I. A critical appraisal to the decision by the company Zimmer Biomet to withdraw the the MaestroTM Wrist Reconstructive System from the marketplace. Trauma Emerg Care. 2018; 3(2):1-10.
Batmanabane M, Malathi S. Movements at the carpometacarpal and metacarpophalangeal joints of the hand and their effect on the dimensions of the articular ends of the metacarpal bones. Anat Rec. 1985;213(1):102-10.
Schmidt I. Update to the difficulties in diagnostic and therapeutic management of the rare carpometacarpal joint II-V dislocation injuries: Case presentation and review of literature. Trauma Emerg Care. 2021;6:1-6.
Dellacqua D. Total Wrist Arthroplasty. Tech Orthop. 2009:24(1):49-57.
Elbuluk AM, Milone MT, Capo JT, Bosco JA, Klifto CS. Trends and Demographics in the Utilization of Total Wrist Arthroplasty. J Hand Surg Asian Pac Vol. 2018;23(4):501-5.
Dafydd M, Whitaker S, Murison MS, Boyce DE. Change in operative workload for rheumatoid disease of the hand: 1,109 procedures over 13 years. J Plast Reconstr Aesthet Surg. 2012;65(6):800-3.
Weiss AP, Akelman E. Total wrist replacement. Med Health R I. 2012;95(4):117-9.
Reigstad O, Holm-Glad T, Bolstad B, Grimsgaard C, Thorkildsen R, Røkkum M. Five- to 10-Year Prospective Follow-Up of Wrist Arthroplasty in 56 Nonrheumatoid Patients. J Hand Surg Am. 2017;42(10):788-96.
Schmidt I. Does Total Wrist Arthroplasty for Treatment of Posttraumatic Wrist Joint Osteoarthritis in Young Patients Always Lead to Restriction of High-demand Activities of Daily Living? Case Report and Brief Review of Recent Literature. Open Orthop J. 2017;11:439-46.
Johnson BM, Flynn MJ, Beckenbaugh ED. A dynamic splint for use after total wrist arthroplasty. Am J Occup Ther. 1981;35(3):179-84.
Schmidt I. Patient Selection in TWA – How Young Can One Go? 74th Annual Meeting of the American Society for Surgery of the Hand (ASSH), Las Vegas 2019 (Instructional Course Lecture 41, 09/06/2019, https://www.researchgate.net/publication/334041603_Patient_Selection_in_TWA_-_How_Young_Can_One_Go_ASSH_Annual_Meeting_2019_Las_Vegas_Speech_Presentation_Last_Update_Oct_31_2021)
Sagerfors M, Gupta A, Brus O, Pettersson K. Total Wrist Arthroplasty: A Single-Center Study of 219 Cases With 5-Year Follow-up. J Hand Surg Am. 2015;40(12):2380-7.
U.S. Food & Drug Administration, 2009: MAUDE Adverse Event Report: BIOMET ORTHOPEDICS MAESTRO TOTAL WRIST DISTAL RADIAL BODY 7.5 MM LEFT PROSTHESIS, WRIST. Biomet Orthopedics.
U.S. Food & Drug Administration, 2012. MAUDE Adverse Event Report: SMALL BONE INNOVATIONS, INC. REMOTION TOTAL WRIST PROSTHESIS, WRIST.
Kandemir G, Smith S, Schmidt I, Joyce TJ. Explant analysis of a MaestroTM wrist prosthesis and calculation of its lubrication regime. J Mech Behav Biomed Mater. 2020;110:103933.
Rossello MI, Zotta I, Rossello C, Formica M, Zoccolan A. Total Wrist Arthroplasty with Integra Freedom® Implants: A Pilot Study with a New Evaluation System. Indian J Orthop. 2022;56(6):1040-7.
Zijlker HJA, Ritt MJPF, Beumer A. Fourth-Generation Total Wrist Arthroplasty: A Systematic Review of Clinical Outcomes. J Wrist Surg. 2021;eFirst.
Zhu XM, Perera E, Gohal C, Dennis B, Khan M, Alolabi B. A systematic review of outcomes of wrist arthrodesis and wrist arthroplasty in patients with rheumatoid arthritis. J Hand Surg Eur Vol. 2021;46(3):297-303.
Dacombe PJ, Amirfeyz R, Davis T. Patient-Reported Outcome Measures for Hand and Wrist Trauma: Is There Sufficient Evidence of Reliability, Validity, and Responsiveness? Hand (N Y). 2016;11(1):11-21.
Akhbari B, Shah KN, Morton AM, et al. Total Wrist Arthroplasty Alignment and Its Potential Association with Clinical Outcomes. J Wrist Surg. 2021;10(4):308-15.
Rizzo M, Berger RA, Steinmann SP, Bishop AT. Arthroscopic resection in the management of dorsal wrist ganglions: results with a minimum 2-year follow-up period. J Hand Surg Am. 2004;29(1):59-62.
Kuliński S , Gutkowska O , Mizia S , Martynkiewicz J, Gosk J. Dorsal and volar wrist ganglions: The results of surgical treatment. Adv Clin Exp Med. 2019;28(1):95-102.
Kamal RN, Ruch DS. Volar Capsular Release After Distal Radius Fractures. J Hand Surg Am. 2017;42(12):1034.e1-1034.e6.
Kane PM, Vopat BG, Mansuripur PK, et al. Relative Contributions of the Midcarpal and Radiocarpal Joints to Dart-Thrower's Motion at the Wrist. J Hand Surg Am. 2018;43(3):234-40.
Gupta A. Total wrist arthroplasty. Am J Orthop (Belle Mead NJ). 2008;37(8 Suppl 1):12-6.
Schmidt I. RE-MOTIONTM total wrist arthroplasty for treatment of advanced stage of scaphoid non-union advanced collapse. Does excision of the entire scaphoid bone prevent impingement at terminal range of radial deviation? Trauma Emerg Care. 2017;2(2):127.
Froschauer SM, Holzbauer M, Hager D, Kwasny O, Duscher D. Proximal Row Carpectomy with Total Scapoidectomy vs. Conventional Carpal Resection for ReMotion Total Wrist Arthroplasty. J Clin Med. 2021;10:1865.
Calendruccio JH. Proximal Row Carpectomy. J Am Soc Surg Hand. 2001;1(2):112-22.
Hung WC, Wang JP, Huang YC, Yin CY, Wu CY, Huang HK. Arthroscopic-assisted radiocarpal ligaments tensioning for dynamic radiocarpal instability. BMC Musculoskelet Disord. 2022;23:158.
Egol KA, Sugi MT, Ong CC, Montero N, Davidovitch R, Zuckerman JD. Fracture site augmentation with calcium phosphate cement reduces screw penetration after open reduction-internal fixation of proximal humeral fractures. J Shoulder Elbow Surg. 2012;21(6):741-8.
Shea TM, Laun J, Gonzalez-Blohm SA, et al. Designs and techniques that improve the pullout strength of pedicle screws in osteoporotic vertebrae: current status. Biomed Res Int. 2014;2014:748393.
Rai AK, Goel R, Bhatia C, Singh S, Thalanki S, Gondane A. Cement Augmentation of Dynamic Hip Screw to Prevent Screw Cut Out in Osteoporotic Patients with Intertrochanteric Fractures: A Case Series. Hip Pelvis. 2018;30(4):269-75.
Schmidt I, Beylich T. „Off label“ use of the ReMotionTM total wrist for treatment of advanced stage of post-traumatic pancarpal wrist osteoarthritis: Report of two cases and review of literature. Trauma Emerg Care. 2020;5:1-9.
Hatano H, Morita T, Kobayashi H, Otsuka H. A ceramic prosthesis for the treatment of tumours of the distal radius. J Bone Joint Surg Br. 2006;88(12):1656-8.
Szczęsny G, Kopec M, Politis DJ, Kowalewski ZL, Łazarski A, Szolc T. A Review on Biomaterials for Orthopaedic Surgery and Traumatology: From Past to Present. Materials (Basel). 2022;15(10):3622.
Fisher P, Sagerfors M, Jacobsson H, Pettersson K. Total Wrist Arthroplasty: A 10-Year Follow-Up. J Hand Surg Am. 2020;45(8):780.e1-780.e10.
U.S. Food & Drug Administration, 2017: MAUDE Adverse Event Report: INTEGRA LIFE SCIENCES CORPORATION UNIVERSAL 2 UNIVERSAL TOTAL WRIST SYSTEM.
Marinello PG, Peers S, Bafus BT, Evans PJ. Modified brachioradialis wrap for stabilizing the distal radioulnar joint: case report. Hand (N Y). 2015;10(4):802-6.
Nunez Jr Fa, Wright A, Kilpatrick Se, Seitz Jr WH. Revision Total Wrist Arthroplasty Due to Polyethylene Wear, Metallosis-Induced Carpal Tunnel Syndrome, Distal Ulnar Impingement, and Fourth Carpometacarpal Joint Pain: Case Report and Pitfalls to Avoid. Hand (N Y). 2020;15(1):NP1-NP6.
Martínez Villén G, Rodríguez Nogué L, García González E. Postoperative assessment and management of metallosis and periprosthetic osteolysis in patients treated with metal-on-polyethylene total wrist prostheses. J Hand Surg Eur Vol. 2022; 47(9):952-958.
Pfanner S, Munz G, Guidi G, Ceruso M. Universal 2 Wrist Arthroplasty in Rheumatoid Arthritis. J Wrist Surg. 2017;6(3):206-15.
Ocampos M, Corella F, del Campo B, Carnicer M. Component alignment in total wrist arthroplasty: success rate of surgeons in their first cases. Acta Orthop Traumatol Turc. 2014;48(3):259-61.
Brumfield RH, Champoux JH. A biomechanical study of normal functional wrist motion. Clin Orthop Relat Res. 1984;(187):23-5.
Gislason MK, Foster E, Bransby-Zachary M, Nash DH. Biomechanical analysis of the Universal 2 implant in total wrist arthroplasty: a finite element study. Comput Methods Biomech Biomed Engin. 2017;20(10):1113-21.
Boeckstyns ME, Herzberg G. Periprosthetic osteolysis after total wrist arthroplasty. J Wrist Surg. 2014;3(2):101-6.
Boeckstyns ME, Toxvaerd A, Bansal M, Vadstrup LS. Wear particles and osteolysis in patients with total wrist arthroplasty. J Hand Surg Am. 2014;39(12):2396-404.
Herzberg G. Periprosthetic bone resorption and sigmoid notch erosion around ulnarhead implants: a concern? Hand Clin. 2010;26(4):573-7.
Brogren E, Abramo A, Tägil M. Bone Remodeling after Ulna Head Replacement in Distal Radioulnar Joint Arthroplasty: A Radiographic Comparison between a Partial and a Total Ulna Head Concept. J Wrist Surg. 2021;eFirst:
Brannan PS, Ward WA, Gaston RG, Chadderdon RC, Woodside JC, Connell B. Two-Year Clinical and Radiographic Evaluation of Scheker Prosthesis (Aptis) Distal Radioulnar Joint Arthroplasty. J Hand Surg Am. 2022;47(3):290.e1-290.e11.
Gvozdenovic R, Boeckstyns M, Merser S. Ulnar Head or Total Distal Radioulnar Joint Replacement, Isolated and Combined with Total Wrist Arthroplasty: Midterm Results. J Wrist Surg. 2020;9(5):411-6.
Completo A, Pereira J, Nascimento A, Almeida F. Strain shielding in distal radius after wrist arthroplasty with a current generation implant: An in vitro analysis. J Biomech. 2017;52:169-75.
Cruz-Pardos A, García-Rey E, García-Cimbrelo E. Total Hip Arthroplasty with Use of the Cementless Zweymüller Alloclassic System: A Concise Follow-up, at a Minimum of 25 Years, of a Previous Report. J Bone Joint Surg Am. 2017;99(22):1927-31.
Boeckstyns MEH. My personal experience with arthroplasties in the hand and wrist over the past four decades. J Hand Surg Eur Vol. 2019;44(2):129-37.
Matsui Y, Minami A, Kondo M, Ishikawa J, Motomiya M, Iwasaki N. A Minimum 5-Year Longitudinal Study of a New Total Wrist Arthroplasty in Patients With Rheumatoid Arthritis. J Hand Surg Am. 2020;45(3):255.e1-255.e7.
Pinder EM, Chee KG, Hayton M, Murali SR, Talwalkar SC, Trail IA. Survivorship of Revision Wrist Replacement. J Wrist Surg. 2018;7(1):18-23.
Fischer P, Sagerfors M, Brus O, Pettersson K. Revision Arthroplasty of the Wrist in Patients With Rheumatoid Arthritis, Mean Follow-Up 6.6 Years. J Hand Surg Am. 2018;43(5):489.e1-489.e7.
Wagner ER, Srnec JJ, Fort MW, Barras LA, Rizzo M. Outcomes of Revision Total Wrist Arthroplasty. J Am Acad Orthop Surg Glob Res Rev. 2021;5(3):e21.00035.
Reigstad O, Holm-Glad T, Thorkildsen R, Grimsgaard C, Røkkum M. Successful conversion of wrist prosthesis to arthrodesis in 11 patients. J Hand Surg Eur Vol. 2017;42(1):84-9.
Zijlker HJA, Fakkert RK, Beumer A, IJsselstein CB, Wessels M, Ritt MJPF. Comparative outcomes of total wrist arthrodesis for salvage of failed total wrist arthroplasty and primary wrist arthrodesis. J Hand Surg Eur Vol. 2022;47(3):302-7.
Swärd EM, Brodda-Jansen G, Schriever TU, Andersson-Franko M, Wilcke MK. The impact of psychological factors on outcome after salvage surgery for wrist osteoarthritis. J Hand Surg Eur Vol. 2022;17531934221104603.
Hoogendam L, van der Oest MJW, Souer JS, Selles RW, Hovius SER, Feitz R, Hand Wrist Study Group. Involvement in a Personal Injury Claim Is Associated With More Pain and Delayed Return to Work After Elective Nonsurgical or Surgical Treatment for Hand or Wrist Disorders: A Propensity Score-matched Comparative Study. Clin Orthop Relat Res. 2022 Sept. 26;doi:10.1097/CORR.0000000000002410. Online ahead of print.
Clough OT, Lee G, Hayter E, Hardman J, Anakwe RE. Surgery with the Motec total wrist replacement: learning from earlier designs. J Surg Case Rep. 2021(1):rjaa560.
Reigstad O, Røkkum M. Wrist arthroplasty using prosthesis as an alternative to arthrodesis: design, outcomes and future. J Hand Surg Eur Vol. 2018;43(7):689-99.
Karjalainen T, Pamilo K, Reito A. Implant Failure After Motec Wrist Joint Prosthesis Due to Failure of Ball and Socket-Type Articulation-Two Patients With Adverse Reaction to Metal Debris and Polyether Ether Ketone. J Hand Surg Am. 2018;43(11):1044e1.-1044e4.
Holm-Glad T, Røkkum M, Röhrl SM, Roness S, Godang K, Reigstad O. A randomized controlled trial comparing two modern total wrist arthroplasties : improved function with stable implants, but high complication rates in non-rheumatoid wrists at two years. Bone Joint J. 2022; 104-B(10):1132-41.
Ota M, Matsui Y, Kawamura D, Urita A, Endo T, Iwasaki N. Correlation between carpal rotational alignment and postoperative wrist range of motion following total wrist arthroplasty. BMC Musculoskeletal Disord. 2022;23(1):821.
Culp RW, Bachoura A, Gelman SE, Jacoby SM. Proximal row carpectomy combined with wrist hemiarthroplasty. J Wrist Surg. 2012;1(1):39-46.
Boyer JS, Adams B. Distal radius hemiarthroplasty combined with proximal carpectomy: case report. Iowa Orthop. 2010;30:168-73.
Bellemère P. Pyrocarbon implants for the hand and wrist. Hand Surg Rehabil. 2018;37(3):129-54.
Vance MC, Packer G, Tan D, Crisco JJ, Wolfe SW. Midcarpal hemiarthroplasty for wrist arthritis: rationale and early results. J Wrist Surg. 2012;1(1):61-8.
Anneberg M, Packer G, Crisco JJ, Wolfe S. Four-Year Outcomes of Midcarpal Hemiarthroplasty for Wrist Arthritis. J Hand Surg Am. 2017;42(11):894-903.
Roux JL. Replacement and resurfacing prosthesis of the distal radius: a new therapeutic concept. Chir Main. 2009;28(1):10-7.
Herzberg G, Burnier M, Marc A, Izem Y. Primary Wrist Hemiarthroplasty for Irreparable Distal Radius Fracture in the Independent Elderly. J Wrist Surg. 2015;4(3):156-63.
Ichihara S, Díaz JJ, Peterson B, Facca S, Bodin F, Liverneaux P. Distal Radius Isoelastic Resurfacing Prosthesis: A Preliminary Report. J Wrist Surg. 2015;4(3):150-5.
Benedikt S, Kaiser P, Schmidle G, Kastenberger T, Stock K, Arora R. Lessons learned with the Cobra prosthesis in elderly patients with complex distal radius fractures-a retrospective follow-up study. Arch Orthop Trauma Surg. 2022;142(2):343-53.
Filippo M, Driessen A, Colarossi G, Quack V, Tingart M, Eschweiler J. Bipolar versus monopolar hemiarthroplasty for displaced femur neck fractures: a meta-analysis study. Eur J Orthop Surg Traumatol. 2020;30(3):401-10.
Gaspar MP, Lou J, Kane PM, Jacoby SM, Osterman AL, Culp RW. Complications Following Partial and Total Wrist Arthroplasty: A Single-Center Retrospective Review. J Hand Surg Am. 2016;41(1):47-53.e4.
Huish EG Jr, Lum Z, Bamberger HB, Trzeciak MA. Failure of Wrist Hemiarthroplasty. Hand (N Y). 2017;12(4):369-75.
Supplementary Information
Video 1:
31-year-old male, Maestro left wrist, 7-year follow-up, well functioning circumduction.
Video 2:
Same patient as in video 1, high load in his occupational work.
Video 3:
Same patient as in videos 1 and 2, high load in his leisure.
Video 4:
Same patient as in videos 1-3, use of a orthotic device imitating TWA.
Video 5:
59-year-old female (Figure 6), ReMotion and uHead left wrist, 9-year follow-up, well functioning circumduction.
Video 6:
Same patient as in video 5 (Figure 6), well functioning „dart thrower’s“ motion.
Video 7:
39-year-old male (Figure 7), ReMotion left wrist, 2-year follow-up, well functioning circumduction.
Video 8:
Same patient as in video 7 (Figure 7), impaired „dart thrower’s“ motion
Video 9:
62-year-old male (Figures 5 and 8), ReMotion and uHead left wrist, 11-year follow-up, well functioning circumduction.
Video 10:
51-year-old female (Figure 10), Maestro right wrist, 6-year follow-up, well functioning circumduction.
Video 11:
Same patient as in video 10 (Figure 10), well functioning „dart thrower’s“ motion.
Video 12:
59-year-old female, ReMotion left wrist, 8-year follow-up, well functioning circumduction (feature of the ReMotion: 10° rotation of the intercalated PE ball against the carpal component).